BLOG & STORIES
Drug Primer: Alpha-PHPP (PV8), Alpha-PiHPP (Iso-PV8), and Alpha-PipHP
By Kevin G. Shanks, D-ABFT-FT
We’ve covered many stimulants on this blog in the past. Most recently, we discussed newer substituted cathinones, MDPHP and Alpha-PHP/PiHP.
As a brief summary, substituted cathinones are a class of compounds that are related to cathinone, a naturally occurring stimulant alkaloid found in the plant Catha edulus (khat). These stimulants first appeared in the USA in the early 2010s and continue to be detected year after year in seized drug evidence and forensic toxicology specimens. MDPHP and alpha-PHP/PiHP (Figure 1) belong to the pyrrolidinophenone subclass of substituted cathinones and are structurally related to older compounds MDPV and alpha-PVP.
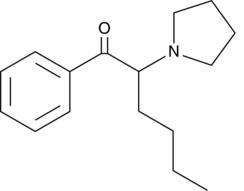
Figure 1. Chemical Structure of Alpha-PHP Drawn by Kevin G. Shanks (2026)
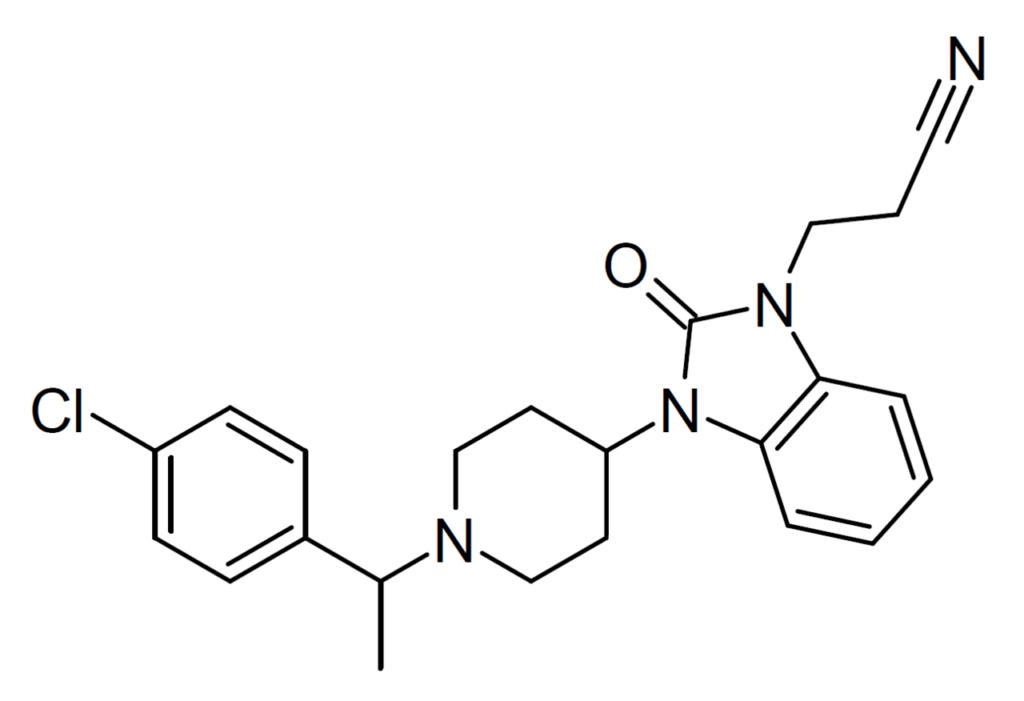
Over the last year, two new compounds (alpha-PHPP and alpha-PiHPP) in the pyrrolidinophenone subclass and one in a related subclass (alpha-PipHP) emerged on the illicit drug market in the USA. As is normal, these compounds have very complex names with some of them also going by alternative names or acronyms. Alpha-PHPP is also known as alpha-pyrrolidinoheptiophenone or PV8. Alpha-PiHPP is also known as alpha-pyrrolidinoisoheptanophenone or iso-PV8 (Figure 2). Alpha-PipHP is also known as alpha-piperidonhexanophenone.
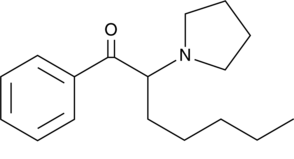
Figure 2. Chemical Structure of Iso-PV8 Drawn by Kevin G. Shanks (2026)
The pyrrolidinophenone compounds differ from other cathinones by incorporating a pyrrolidine ring and often a longer alkyl side chain, while alpha-PipHP is structurally related to older cathinones, alpha-PHP and alpha-PiHP. Though the published pharmacology literature remains sparse, rather than functioning primarily as monoamine releasing agents, compounds with similar chemical structures as these three stimulants typically act as potent inhibitors of dopamine and norepinephrine transporters. This makes them function in a similar fashion to cocaine but with greater potency and longer durations of action. This pharmacological action of transporter inhibition leads to elevated extracellular dopamine in the neuronal synapse and contributes to increased locomotor activity, euphoria, reinforcement, and abuse liability. Increased norepinephrine in the synapse contributes to sympathetic activation, including tachycardia, hypertension, hyperthermia, and heightened alertness. The severity of toxicity varies widely depending on factors such as dose, route of administration, co-administration of other substances, health or disease state of the user, and the use history of the individual. Expected metabolism and excretion of these compounds includes reduction, hydroxylation, oxidation, and conjugation with glucuronic acid or sulfate.
There have been a couple of reports over the last decade of the detection of PV8 in postmortem casework outside of the USA.
In 2018, Pieprzyca et al. reported two fatal cases involving PV8 in Japan. In the first case, a 36 year old man was found dead in his apartment. The previous night he had consumed alcohol with friends. Blood was positive for ethanol (1.8 mg/L), clindamycin (1.95 mcg/mL), and PV8 (0.26 mcg/mL). In the second case, a 37 year old female arrived at the hospital with gastrointestinal bleeding, vomiting, diarrhea, hyponatremia, and hypokalemia. Postmortem blood was acetaminophen (1.49 mcg/mL), metamizole (0.32 mcg/mL), lidocaine (0.68 mcg/mL), dextromethorphan (0.28 mcg/mL), drotaverine (0.25 mcg/mL), and PV8 (0.07 mcg/mL). Both deaths were concluded to be fatal intoxications with PV8.
In 2021, Mochizuki et al. described a fatal case of poisoning with PV8, alongside other stimulants 4-FMC, 4-MeO-alpha-PVP, and 4-F-alpha-PVP. The male decedent was found without clothes in his room and with his head embedded in the wall. A syringe and vials of liquid were also found in the room. PV8 was quantified in postmortem heart blood (218±3 ng/mL) and in postmortem femoral blood (167±4 ng/mL). 4-FMC, 4-MeO-alpha-PVP, and 4-F-alpha-PVP were also quantified in both samples. The authors concluded the cause of death to be acute poisoning with the combination of substances detected.
As these compounds are now on the illicit drug market, it is prudent to be aware of them. Axis monitors alpha-PipHP, Alpha-PHPP (PV8), and Alpha-PiHPP (iso-PV8) in the Novel Emerging Compounds (NEC) panel (order code 13710) and Comprehensive Panel, Blood with Analyte Assurance™ (order code 70510) using liquid chromatography with quadrupole time of flight mass spectrometry (LC-QToF-MS). Since the addition to the scope of testing in April 2026, the laboratory has detected alpha-PiHPP (iso-PV8) in 4 postmortem blood cases. Each of the cases originated in the state of Florida. Of the four cases, 2 decedents were female and 2 decedents were male. Other drugs detected alongside alpha-PiHPP (iso-PV8) included cocaine/metabolites (2), fentanyl/metabolite (2), and methamphetamine/amphetamine (2). Alpha-PipHP and Alpha-PHPP (PV8) have not been detected in the laboratory.
If you have any questions or concerns about these new stimulants and how they may play a role in your medical-legal investigation, please reach out to subject matter experts by email ([email protected]) or phone (317-759-4869, Option 3).
References
- Shanks, K. (2026) Drug Primer: MDPHP. https://axisfortox.com/drug-primer-mdphp/
- Shanks, K. (2023) Poster Presentation: Detection of the Substituted Cathinone, Alpha-PiHP, in Postmortem Toxicology Cases. https://axisfortox.com/poster-presentation-detection-of-the-substituted-cathinone-alpha-pihp-in-postmortem-toxicology-cases/
- Shanks, K. (2023) A Closer Look at the Novel Emerging Compounds Panel: Alpha-PiHP and N,N-dimethylpentylone. https://axisfortox.com/a-closer-look-at-the-novel-emerging-compounds-panel-alpha-pihp-and-nn-dimethylpentylone/
- Pieprzyca, E., Skowronek, R., Korczynska, M., Kulikowska, J., and Chowaniec, M. (2018) Two fatal cases of poisoning involving new cathinone derivative PV8. Legal Medicine (Tokyo). https://doi.org/10.1016/j.legalmed.2018.05.002.
- Mochizuki, A., Adachi, N., and Shojo, H. (2021) Detection of 4-FMC, 4-MeO-α-PVP, 4-F-α-PVP, and PV8 in blood in a forensic case using liquid chromatography-electrospray ionization linear ion trap mass spectrometry. Forensic Science International. https://doi.org/10.1016/j.forsciint.2021.110888.
Axis Forensic Toxicology Recognized by ANAB for Accreditation Renewal
In forensic toxicology, confidence in a result is built long before a report is issued.
It is built through validated methods, documented processes, trained people, careful review, quality systems, and a shared commitment to doing the work the right way.
Axis Forensic Toxicology is grateful to be recognized by ANAB – ANSI National Accreditation Board for the renewal of our accreditation to American Board of Forensic Toxicology and ISO/IEC 17025:2017 standards in the field of Forensic Testing, Toxicology.
ISO/IEC 17025:2017 is an internationally recognized standard for laboratory competence, quality systems, and technically valid testing. In forensic toxicology, that rigor matters. The clients we serve often rely on toxicology results in serious, sensitive, and consequential matters. That responsibility calls for more than scientific capability. It calls for disciplined systems, consistent practices, and a culture committed to quality.
Dr. Laureen Marinetti, Chief Toxicologist at Axis, sees accreditation as part of the responsibility forensic toxicology carries. Trust in a result is built one careful step at a time — through the methods used, the reviews performed, and the way each case is approached.
For Axis, accreditation is not simply a credential. It reflects the daily discipline required to serve clients well.
Much of that work happens behind the scenes — in the procedures we follow, the documentation we maintain, the training we complete, the reviews we perform, and the continuous improvement that supports our laboratory each day.
Accreditation renewal also reflects steady, shared work across the organization. Much of that work is not visible to clients, but it matters to every result Axis reports. That is how Matt Zollman, Director of Operations and Product Management at Axis, describes the operational discipline behind the renewal.
This recognition reflects the people behind Axis — the team members who receive, prepare, test, review, report, support, document, audit, correct, improve, and serve. Their work is often unseen, but essential to the clarity and confidence our clients need when toxicology results become part of a larger case record.
Axis appreciates ANAB’s recognition and the continued opportunity to uphold these standards in forensic toxicology.
Most of all, Axis is grateful for the team whose daily discipline makes this standard real in the work we do for clients.
Read MoreAxis Toxicologists Provide Practical Training at Kentucky Coroner’s Association Annual Meeting

From left to right: Dr. Marinetti, Mr. Kurtz, Mr Shanks.
MATT 2026 Recap: Mitragynine Pseudoindoxyl
In March, Stuart Kurtz presented at the 2026 annual meeting of the Midwest Association of Toxicology and Therapeutic Drug Monitoring (MATT) on kratom products and how they’ve changed over the years. Previous blog posts have discussed mitragynine, kratom case reports, and the emergence of 7-OH mitragynine. Mitragynine pseudoindoxyl is the latest variation to be sold and used by kratom users.
As a quick recap, kratom is a plant that occurs naturally in many parts of Southeast Asia and is commonly consumed by chewing leaves or brewing tea. Mitragynine is the primary alkaloid in the plant material. 7-OH mitragynine (7OH) occurs naturally but at much lower concentrations, and is approximately 10x more potent than mitragynine. It has CNS stimulant effects at lower doses and CNS depressant effects at higher doses. While not regulated at the federal level in the United States, states can decide if they want to regulate sale, possession, and use.
Products containing mitragynine pseudoindoxyl (MPI) have emerged in the past 2 years. MPI is about 10x more potent than 7OH and 100x more potent than mitragynine. MPI is not often found in kratom plant material at detectable levels. In toxicology testing, MPI can be found as a metabolite and breakdown product of the naturally occurring 7OH. Because it’s also a breakdown product of 7OH, products containing 7OH can contain varying amounts of MPI that may not be intended by the manufacturer for consumption by the user.

Sellers from left to right, top to bottom: CBD American Shaman, Real Botanicals, Bulk Kratom Capsules (BKC), Pure Leaf Kratom
Products can also be manufactured to intentionally contain MPI in them. These, like 7OH products, are not extracts of kratom plant material. The mitragynine from the kratom plant is extracted and synthetically converted to 7OH and/or MPI. These products may contain much more active components than kratom plant material and, due to lack of regulation, the products may vary in concentration from batch to batch of the same product.
Interpretation of cases containing kratom alkaloids can be tricky. Quantitative data is currently being collected by some labs to help establish expected ratios of mitragynine, 7OH, and MPI in kratom plant material exposure vs. 7OH and MPI product exposure. Toxicology results from 7OH and MPI product exposures might have little or no mitragynine present. Simply screening for mitragynine may result in cases being missed.
7OH is a very small component of the kratom plant material so exposure to it is not likely to have detectable amounts of 7OH or MPI. Large amounts of kratom plant exposure can lead to detectable 7OH and MPI since 7OH is naturally occurring and a metabolite of mitragynine with MPI as a metabolite of 7OH. Relatively low concentrations of mitragynine and the presence of 7OH and/or MPI may indicate exposure to a product that contains 7OH and/or MPI. Scene evidence such as product packets or web browser search history can be helpful in these cases.
Presence of 7OH and/or MPI is notable from a toxicology perspective and inclusion of all known kratom alkaloids in a case on the death certificate can help with public health tracking. It is encouraged to discuss these cases with a toxicologist when they arise to make sure all possibilities are considered. There may be insufficient information available to determine if the exposure was kratom plant material, synthetically converted product, or a combination.
For any questions or assistance with interpretation, please email us at [email protected] or give us a call at 317-759-4869 option 3.
References
- George S Behonick, Christina Vu, Larry Czarnecki, Maisie El-Ters, Kevin G Shanks, Two Single-Drug Fatal Intoxications by Mitragynine, Journal of Analytical Toxicology, Volume 46, Issue 5, June 2022, Pages e110–e114, https://doi.org/10.1093/jat/bkac016
- Sanderson, Mark; Rowe, Adrianna. Kratom. CMAJ Oct2019, 191 (40) E1105; DOI: 10.1503/cmaj. 190470
- Afzal H, Esang M, Rahman S. A Case of Kratom-induced Seizures. Cureus. 2020 Jan 7;12(1):e6588. doi: 10.7759/cureus.6588. PMID: 32051800; PMCID: PMC7001130.
- Krotulski, AJ; Denn, MT; Brower, JO; Papsun, DM; Logan, BK. (2025), Evaluation of Commercially Available Smoke Shop Products Marketed as “7-Hydroxy Mitragynine” & Related Alkaloids, Center for Forensic Science Research and Education, United States.
- Anderer S. What to Know About 7-OH, the New Vape Shop Hazard. JAMA. 2025;334(12):1045–1046. doi:10.1001/jama.2025.13592
- Smith, K.E., Boyer, E.W., Grundmann, O., McCurdy, C.R. and Sharma, A. (2025), The rise of novel, semi-synthetic 7-hydroxymitragynine products. Addiction, 120: 387-388. https://doi.org/10.1111/add.16728
- Pullman MK, Kanumuri SRR, Leon JF, Cutler SJ, McCurdy CR, Sharma A. Cardio-pulmonary arrest in a patient revived with naloxone following reported use of 7-hydroxymitragynine. Clin Toxicol (Phila). 2025 Sep 30:1-2. doi: 10.1080/15563650.2025.2565428. Epub ahead of print. PMID: 41025553.
Why “A Decade of Clarity”
![]()
In 2026, Axis Forensic Toxicology marks ten years as Axis.
To recognize that milestone, we have chosen a simple anniversary theme: A Decade of Clarity.
That phrase is not meant to be a slogan layered on top of the work. It is meant to name something true about the work itself.
For Axis, this anniversary is about more than time passed. It is about what ten years have held. It is about what has been built, what has been refined, and what has been strengthened through steady attention over time. It is about ten years of building, evolving, and investing in the science, service, and relationships that matter most to the forensic community.
From the beginning, clarity has mattered here.
Clarity matters in the laboratory. It matters in the integrity of the science, in the discipline of the methods, and in the responsibility to produce results that are sound, defensible, and useful.
Clarity also matters in service. At Axis, our service model has been built around direct access to experts — thoughtful, informed support from people who understand the science and the realities of casework. That kind of support requires discernment. It requires listening carefully, responding intentionally, and helping clients navigate complexity with confidence.
And clarity matters in stewardship. Over the years, Axis has continued investing in tools and capabilities that help clients not only detect what matters, but do so with purpose. Analyte Assurance is one example of that approach — an effective way to strengthen detection while also helping steward budgets responsibly.
That is part of why this theme feels fitting.
Over the past decade, Axis has continued building a strong laboratory and service model. We have evolved with the needs of the field, with the realities of changing casework, and with the scientific demands of a shifting drug landscape. We have invested in people, instrumentation, systems, and capabilities that strengthen both the work and the support behind it.
None of that happens all at once. It happens over time. It happens through discipline, through care, and through a long pattern of choosing to keep building.
That is what this anniversary reflects.
A Decade of Clarity is not simply a way of marking ten years in business. It is a way of honoring what those ten years have required and what they have made possible. It is a way of naming the work of building something steady, useful, and trusted.
We are grateful for the clients, colleagues, and partners who have been part of this journey. And we are thankful for the opportunity to continue the work.
For Axis, ten years is not just a milestone to celebrate across a year. It is a continuing expression of how we aim to serve — with clarity, steadiness, and thoughtful partnership in work that matters.
Read MoreMATT 2026 Recap: BTMPS
Axis toxicologists Laureen Marinetti, PhD, F-ABFT, and Stuart Kurtz, M.S, D-ABFT-FT, presented at the Midwest Association of Toxicology and Therapeutic Drug Monitoring (MATT) Annual Meeting in Cincinnati, Ohio, March 18-20, 2026. A recap and update of Dr. Marinetti’s presentation follows.
Dr. Marinetti presented on BTMPS, (Bis[2,2,6,6-tetramethyl-4-piperidyl] sebacate), brand name Tinuvin®770, at the 2026 Midwest Association for Toxicology and Therapeutic Drug Monitoring annual meeting (MATT) in Cincinnati Ohio on March 19. BTMPS is commonly used in the manufacture of plastics as a UV‑stabilizing additive. While BTMPS is often found in samples alongside fentanyl, synthetic opioids, and stimulants, it can also be found in the absence of these typical illicit drugs. Axis has identified two positive cases with BTMPS without the presence of illicit drugs in blood, and four cases with the presence of illicit drugs. The cases without illicit drugs were an oxycodone overdose with a very high concentration of oxycodone, and an Adderall overdose with a large concentration of amphetamine. One decedent had filled a prescription for 120 oxycodone pills, the next day he was found deceased and all of the oxycodone pills were gone. In the second case the decedent had a prescription for 90 Adderall pills with none remaining. In addition, Axis became aware of a third case involving an individual that was subject to urine testing due to pain management therapy. The urine test results matched the prescriptions the individual was taking with no illicit drugs present, and he was therefore considered compliant. However BTMPS was also detected in the urine sample. In addition, a laboratory in Ohio reported the seizure of 200 illicit M30 pills, which upon testing, only contained BTMPS.
A question of how the BTMPS entered the licit drug supply was discussed at the MATT meeting. It is possible that the BTMPS was a contaminant on the oxycodone pills from the plastic medication bottle(s) in which they were stored since manufacture or from an ingredient used to manufacture the pills, and because so many of them were ingested at one time, the BTMPS accumulated to a detectable concentration. For the individual in pain management therapy, he was on multiple medications most of which were stored in plastic bottles, including an opioid.
The University of Washington drug detection data showed that in licit drug samples, BTMPS was detected. In 311 prescription opioid samples (excluding fentanyl), 3.5% were positive for BTMPS, thus supporting the BTMPS leaching out of the plastic containers during pill storage or manufacture.
Further evidence that the BTMPS may be leaching out of plastic was found. BTMPS is a potent calcium channel blocker and nicotine receptor antagonist. For this reason it has been used in nicotinic receptor studies. It was discovered by Papke et.al, that in the control and the BTMPS treated nicotinic receptors; both produced the same results of receptor blockade. After investigation it was discovered that BTMPS was leaching out of the plastic syringes that were being used. When the plastic syringes were removed from use, the control and BTMPS groups no longer produced the same results.
Because BTMPS has been found in biological specimens from postmortem and ante-mortem samples without the presence of illicit drugs, in prescription opioid pills, and found to leach out of plastic, there can be no assumption that the individual used illicit drugs if BTMPS is confirmed.
If you have any questions or concerns regarding the role of BTMPS or any other newly emerged substance in your investigation, please reach out to our Axis Forensic Toxicology subject matter experts at [email protected] or by phone (317-759-4869, Option 3). To stay current with the scope of testing for all services offered by Axis, please consult the online catalog at https://Axisfortox.com.
References
- Glossman H., Hering, S., Savchenko, A., Berger, W., et.al., A light stabilizer (Tinuvin 770) that elutes from polypropylene plastic tubes is a potent L-type Ca2+-channel blocker. Proc. Natl. Acad. Sci. USA, Vol. 90, pp9523-9527, October 1993.
- Papke, R.L., Craig, A.G., and Heinemann, S.F., Inhibition of nicotinic acetylcholine receptors by bis (2,2,6,6-tetramethyl-4-piperidinyl) sebacate (Tinuvin 770), an additive to medical plastics. J.Pharmacol Exp Ther. 1994 Feb;268(2):718-26.
- UV Stabilizer BTMPS in the Illicit Fentanyl Supply in 9 US Locations, Letter, Journal of the American Medical Association, February 5, 2025.
- Where do we see BTMPS? Addictions, Drug and Alcohol Institute, University of Washington, https://adai.washington.edu/WAdata/DrugChecking/BTMPS.html, 2026.
- The first BTMPS Blog post on the Axis Website Feb 6, 2026. https://axisfortox.com/drug-primer-btmps/
Introducing A Decade of Clarity
![]()
In 2026, Axis Forensic Toxicology marks ten years as Axis.
To recognize that milestone, we are proud to introduce our anniversary theme: A Decade of Clarity.
This theme reflects more than time passed. It reflects ten years of building, evolving, and investing in the science, service, and relationships that matter most to the forensic community.
Since 2016, Axis has remained focused on delivering clear answers in complex cases, responsive support, and continued investment in the people, systems, and capabilities that strengthen our work.
As we move through 2026, A Decade of Clarity will serve as a simple expression of what this milestone means to Axis: not just ten years in business, but ten years of steady commitment to clarity, partnership, and progress.
We are grateful for the opportunity to serve the forensic community and thankful for the clients and partners who have been part of this journey.
Thank you for being part of the Axis story.
Phil Roberts
Chief Executive Officer
Axis Forensic Toxicology
Emerging Substances – The “Orphines” Class of Designer Opioids
By Kevin G. Shanks, D-ABFT-FT
The term designer opioid generally refers to the class of synthetically derived opioid analogs that are intentionally modified by clandestine chemists to circumvent existing drug laws while maintaining opioid receptor activity. This concept has been ongoing over the years with the initial appearance of fentanyl analogs such as alpha-methylfentanyl and 3-methylfentanyl during the 1980s and the reemergence of them on illicit drug markets in the 2010s. Shortly thereafter, the fentanyl class of compounds was heavily controlled by the government, and clandestine labs moved on to the synthesis of the nitazene family of opioids, which gained prominence in the late 2010s to early 2020s. As the nitazenes have become regulated, the market looks to be shifting again, and the orphine class of opioids has the potential to be the next type of designer opioid to become prevalent.
The orphine class of substances have an origin in academic and pharmaceutical research conducted during the 1960s and 1970s, particularly in laboratories associated with Paul Janssen, whose work also produced fentanyl and related fentanyl analogs. Many of these compounds were initially synthesized as potential analgesics, but they remained relatively obscure within scientific literature and patents. In the last few years, these compounds have been rediscovered and have found their way to the street as illicit drugs.
The modern recognition of the orphine class began with the detection of brorphine on illicit drug markets in Europe in 2019 and in the United States in 2020. Brorphine is a benzmidazol-2-one derivative that contains a cyclized benzimidazole ring system. Other compounds in this class include cyclorphine (also known as N-propionitrile chlorphine), and 5,6-dichloro desmethylchlorpine (also known as S-17018), and 5,6-dichloro brorphine (also known as SR-14968).
Chemical Structure of Brorphine Drawn by Kevin G. Shanks (2026)
The other structural group of orphine compounds are the spiropiperidine derivatives, which contain a spiro-linked piperidine ring fused with an imidazole or other related aromatic system. Compounds in this class include spirorphine, spirochlorphine, and spirobrorphine.
The orphines may differ from the traditional morphine derivatives and the typical fentanyl analogs in chemical structure, but the pharmacological effect is similar, as they act as potent mu opioid receptor agonists. This activity produces analgesia, euphoria, sedation, central nervous system depression, and respiratory depression. In overdose, the breathing slows down, and may stop temporarily (apnea). Apnea leads to hypoxia, or lack of oxygen distribution to the surrounding tissues including the brain. Hypoxia can lead to cardiac arrest and death.
Chemical Structure of Cyclorphine Drawn by Kevin G. Shanks (2026)
The orphine class of opioids is particularly concerning from a toxicological perspective as some of the analogs are considered to be high potency, with several of them being similar to fentanyl in pharmacological activity. Many of these compounds have very limited toxicological data as they never underwent routine animal or human clinical testing. Because of these factors and with the potential increased prevalence in drug materials on the street, forensic toxicology laboratories have begun expanding their analytical methods to identify these compounds in postmortem analyses. As always, the cycle of innovation by clandestine chemists and then governmental prohibition drives the continual appearance of new opioids on the drug market. Although only a limited number of analogs have been detected so far, their appearance illustrates how the drug market changes rapidly over the course of months and years.
Axis Forensic Toxicology has been testing for brorphine since 2023 and recently added chlorphine, N-propionitrile chlorphine (cyclorphine), 5,6-dichloro brorphine, 5,6-dichloro desmethylchlorphine, spirobrorphine, and spirochlorphine to a newly developed Orphine Analog Panel (order code 13410), and Comprehensive Panel, Blood with Analyte Assurance™ (order code 70510) using liquid chromatography with quadrupole time of flight mass spectrometry (LC-QToF-MS). Reporting of these analytes is qualitative. Reporting limits are 10 ng/mL for 5,6-dichloro brorphine and 5,6-dichloro desmethylchlorphine and 1 ng/mL for chlorphine, N-propionitrile chlorphine, spirobrorphine, and spirorchlorphine.
If you have any questions or concerns regarding the role of these orphine opioids or any other newly emerged substance in your investigation, please reach out to our Axis Forensic Toxicology subject matter experts at [email protected] or by phone (317-759-4869, Option 3). To stay current with the scope of testing for all services offered by Axis, please consult the online catalog.
Read MoreUpcoming Additions to Comprehensive Panel with Analyte Assurance™ and New Orphine Analog Panel
We’re pleased to inform you that effective April 20th, 2026, Axis will be updating our Comprehensive Panel with Analyte Assurance™ and offering a new Orphine Analog Panel.
What is Changing?
For orders placed on or after April 20th, 2026, the 70510 Comprehensive Panel, Blood will include the following added analytes:
- alpha-PHPP (PV8) – Confirmed via 13710: Novel Emerging Compounds Panel
- alpha-PiHPP (Iso-PV8) – Confirmed via 13710: Novel Emerging Compounds Panel
- alpha-PipHP – Confirmed via 13710: Novel Emerging Compounds Panel
- Ethylbromazolam – Confirmed via 13510: Designer Benzodiazepine Panel
- Mitragynine Pseudoindoxyl – Confirmed via 13710: Novel Emerging Compounds Panel
- N-Pyrrolidino Ethylene Isotonitazene – Confirmed via 13910: Nitazene Analog Panel
- N-Pyrrolidino Isotonitazene – Confirmed via 13910: Nitazene Analog Panel
- Phenazolam – Confirmed via 13510: Designer Benzodiazepine Panel
- Suzetrigine – Provided as part of 70510: Comprehensive Panel, Blood
Additionally, with the rise of “Orphines” throughout the United States, Axis will be offering a new 13410: Orphine Analog Panel, Blood. As with other emerging and designer type panels, the screening for these analytes will be included as part of Analyte Assurance in the 70510: Comprehensive Panel, Blood. The components of this panel are detailed below.
- 5,6-Dichloro Brorphine
- 5,6-Dichloro Desmethylchlorphine
- Brorphine
- Chlorphine
- N-Propionitrile Chlorphine (Cychlorphine)
- Spirobrorphine
- Spirochlorphine
What Do You Need to Do?
You do not need to do anything different as these analytes will automatically be included with your 70510: Comprehensive Panel, Blood order under Analyte Assurance. For a copy of the new specification sheet that is effective April 20th, 2026 please click this link: https://axisfortox.com/test_catalog/comprehensive-drug-panel/
At Axis Forensic Toxicology, we are committed to evolving with the needs of our clients and the ever-changing landscape of emerging substances. These additions reflect our proactive approach to ensuring you receive the most comprehensive and reliable testing services available.
If you have any questions or would like more information regarding this update, please don’t hesitate to reach out to us at [email protected]. Our team is always ready to assist.
Thank you for your continued partnership and trust in Axis. We look forward to continuing to support your work with the highest quality service and testing solutions.
Sincerely,
Matt Zollman
Director of Operations & Product Management
Axis Collaborates with Forensic and Investigative Sciences Program
Axis is fortunate to have strong university science programs within the state of Indiana to supply forensic scientists to work in its laboratory. Axis maintains a particularly strong relationship with the Forensic and Investigative Sciences (FIS) program at Indiana University Indianapolis (formerly Indiana University Purdue University Indianapolis). Axis’ Chief Operating Officer, Denise Purdie Andrews, serves on the FIS Board of Visitors, and Axis’ Director of Operations and Product Management, Matt Zollman, recently served on a panel presentation associated with the recent FIS 20th Anniversary Symposium.
Axis’ longest-standing relationship is with toxicologist Kevin Shanks, who has served from time to time as a speaker and instructor over the past decade. Kevin has also collaborated with its faculty and students on research. This research has culminated with a published paper, “Paper Spray Mass Spectrometry for Rapid Drug and Drug Metabolite Screening Directly from Postmortem Blood Samples”. It is available for review here: https://www.ojp.gov/library/publications/paper-spray-mass-spectrometry-rapid-drug-and-drug-metabolite-screening
Axis is pleased to engage with others in the forensic science community and to support the research efforts of students and faculty in Indiana and beyond.
Read More