By Kevin Shanks, D-ABFT-FT
Pharmacokinetics (PK) is the study of what the body does to a substance. The word is derived from Greek – Pharmakon which means “drug” and kinetikos which means “moving”. PK consists of four areas – absorption, distribution, metabolism, and excretion. This is also known as ADME.

Instrumentation in the Drug Metabolism and Pharmacokinetics Lab “Equipment used in the DMPK Lab” by NIH-NCATS is licensed under CC PDM 1.0.
Absorption (A) is the process by which substances enter the bloodstream. Substances can enter the bloodstream through a wide variety of routes, including oral (by mouth), inhalation (lungs), intravenous (injected into a vein), intramuscular (injected into muscle), rectal (suppository), oral mucosa (under the tongue), intrathecal (spinal fluid), dermal (skin), ocular (eye), and intranasal (nose).
Distribution (D) refers to the transfer of a substance form one part of the body to another. When discussing PK, this usually refers to the movement of substance from the blood into the tissues of the body (liver, heart, kidney, brain, muscle, and fat). Some factors that influence distribution are lipophilicity, pH, and plasma protein binding.
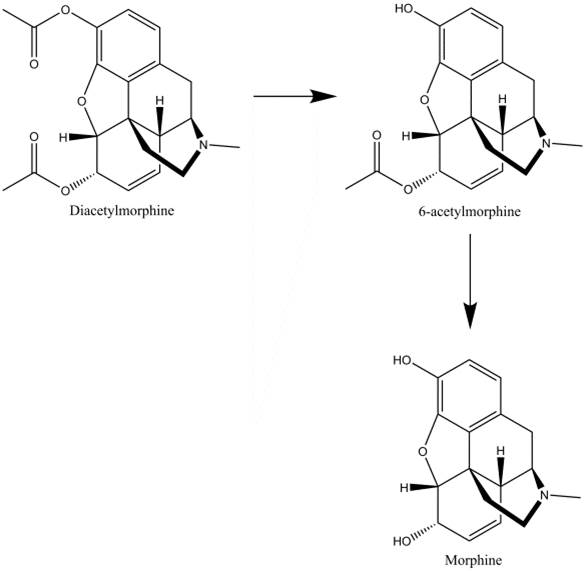
Metabolism of Heroin (Diacetylmorphine) Chemical structures drawn by Kevin G. Shanks (2018)
Metabolism (M) is the process by which the substance is altered to facilitate the removal of it from the body. Most metabolism occurs in the liver, but it can also occur in the kidneys, lung, gastrointestinal tract, and blood. Examples of metabolism include deacetylation (heroin to 6-acetylmorphine to morphine), nitro reduction (clonazepam to 7-aminoclonazepam), N-dealkylation (amitriptyline to nortriptyline), deamination (chlordiazepoxide to demoxepam to nordiazepam), and ester hydrolysis (cocaine to benzoylecgonine), as well as glucuronidation (oxazepam to oxazepam glucuronide), sulfate formation (morphine to morphine sulfate), and glycine conjugation (salicylate to salicyluric acid)
Excretion (E) is the final removal of the substance or by products from the body. Excretion is most commonly done via the liver and kidneys, but can occur via the lungs, breast milk, feces, sweat, sebum, and semen.
PK can help answer questions such as ‘Are drugs involved in this incident?’, ‘How much substance did a living individual consume?’, or ‘When was a substance taken by an individual?’.
The larger question at hand in many cases regarding impairment, drug toxicity, or a substance’s role in cause of death involves a related area of pharmacology called pharmacodynamics (PD), which will be explored in a later blog post.
If you have any questions or concerns regarding the role of pharmacokinetics in your toxicology case, please reach out to our Axis Forensic Toxicology subject matter experts at [email protected].
References
Guidelines for the Interpretation of Analytical Toxicology Results. Disposition of Toxic Drugs and Chemicals in Man. Twelfth Edition. Randall C. Baselt. Biomedical Publications. Pages xxx-xlii. (2020).
Pharmacokinetics and Pharmacodynamics. Principles of Forensic Toxicology. Fourth Edition. Barry Levine. American Association for Clinical Chemistry (AACC). 2017. 77-93.
Introduction to Forensic Toxicology. Clarke’s Analytical Forensic Toxicology. Sue Jickells and Adam Negrusz. Pharmaceutical Press. Pages 1-12. (2008).
Postmortem Toxicology. Clarke’s Analytical Forensic Toxicology. Sue Jickells and Adam Negrusz. Pharmaceutical Press. Pages 191-218. (2008).
Postmortem Forensic Toxicology. Principles of Forensic Toxicology. Fourth Edition. Barry Levine. AACC, Inc. Pages 3-14. (2017).
Alcohol, Drugs, and Driving. Clarke’s Analytical Forensic Toxicology. Sue Jickells and Adam Negrusz. Pharmaceutical Press. Pages 299-322. (2008).
Human Performance Toxicology. Principles of Forensic Toxicology. Fourth Edition. Barry Levine. AACC, Inc. Pages 15-30. (2017).