BLOG & STORIES
A Closer Look at the Novel Emerging Compounds Panel: Phenibut and Tianeptine
By Kevin Shanks, M.S., D-ABFT-FT
As mentioned in previous blog posts, novel psychoactive substances (NPS) come in different varieties and the Novel Emerging Compounds (NEC) Panel offered by Axis Forensic Toxicology helps to detect the most newly emerged NPS on the drug market and is meant to evolve over time as new drugs emerge on the street. In the first post in the series, we took a look at two of the more recently emerged NPS benzodiazepines, bromazolam and flubromazepam, and in the second post, we looked at two of the most recently detected stimulants, alpha-PiHP and N,N-dimethylpentylone. In this third post in the series, we will take a brief look at two more recently emerged compounds: phenibut and tianeptine.
Phenibut is a substance that was originally developed in the Soviet Union in the 1960s and is currently marketed as a medication in Belarus, Kazakhstan, Latvia, Russia, and Ukraine and used in the treatment of anxiety and insomnia, as well as many other disease states and disorders. Phenibut is not approved for use in the United States, but it has been sold on the internet as a dietary supplement and nootropic and has been used recreationally. The name phenibut is derived from the chemical name (B-phenyl-y-aminobutyric acid). It is an analog of the neurotransmitter gamma-aminobutyric acid (GABA) and is thought to act as a GABA receptor agonist (similar to baclofen), but it also has dopaminergic effects. Reported effects of the substance include sedation, tiredness, drowsiness, nausea, headache, irritability, agitation, and euphoria. Phenibut is currently considered an uncontrolled substance in the United States.
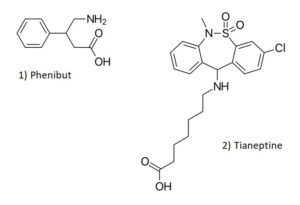
Chemical Structures of Phenibut and Tianeptine
Structures drawn by Kevin G. Shanks (2023).
Tianeptine is a drug that was developed by the French Society of Medical Research in the 1960s and is currently approved as a prescription medication in France and other European and Asian countries. It is used for the treatment of major depressive disorder, as well as anxiety, irritable bowel syndrome, and asthma. Tianeptine is not approved for use in the United States as a medication. It has been found as a drug of abuse throughout the years in Russia and has become an emerging public health risk in the United States as a recreational drug. Tianeptine is a mu opioid receptor agonist and also has glutamate receptor activity via the α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) and N-methyl-D-aspartate (NMDA) receptors. Reported effects of tianeptine use include headache, drowsiness, nausea, agitation, anxiety, and euphoria. Tianeptine is not a controlled substance in the United States, but has been controlled at the state level in Alabama, Michigan, Ohio, and Tennessee as either a Schedule I or II substance.
As both substances are not controlled substances at the Federal level, the Drug Enforcement Administration (DEA) has not released any detection or prevalence data via the National Forensic Laboratory Information System (NFLIS), but both phenibut and tianeptine have been implicated in human toxicity which have led to hospitalizations and have also been associated with fatalities in the United States.
Axis qualitatively monitors both of these compounds in our NEC panel (order code 13710) and Comprehensive Panel, Blood with Analyte Assurance (order code 70510) using liquid chromatography with quadrupole time of flight mass spectrometry (LC-QToF-MS). Over the time range 01/30/2023 – 06/30/2023, Axis has detected phenibut in 5 blood specimens in 5 states (Arizona, Florida, Indiana, Ohio, and Tennessee) and tianeptine in 6 cases in 4 states (Florida, Indiana, Kentucky, and Tennessee). In Axis Forensic Toxicology casework, phenibut was typically found alongside THC/THC-COOH (n=2), tianeptine (n=2), caffeine (n=2), dextromethorphan (n=1), and fentanyl/norfentanyl (n=1). Tianeptine was simultaneously detected with bromazolam (n=2), phenibut (n=2), cotinine (n=2), fentanyl/norfentanyl (n=1), and methamphetamine (n=1).
Axis also monitors other NPS in our Novel Psychoactive Substances panel (order code 13610). These additional compounds include 25B-NBOMe, 25C-NBOMe, 25I-NBOMe, 2C-B, 2C-E, 2C-I, 5-MeO-DALT, adinazolam, alpha-PVP, butylone, clonazolam, dibutylone, dimethylone, ethylone, etizolam, eutylone, flualprazolam, flubromazolam, MDPV, mephedrone, methcathinone, methedrone, methoxetamine, methylone, N-ethylpentylone, pentylone, and TFMPP.
As always, if you have questions about these substances and how they may play a role in your medical-legal investigation, please reach out to our subject matter experts by email ([email protected]) or phone (317-759-4869, Option 3).
Be on the lookout for the fourth and final post in the NEC Panel series! To round out the panel, we will take a brief look at three more recently emerged novel compounds: AP-237, brorphine, and fluorofentanyl.
Read MoreNot Dead Yet: Detection of Carfentanil in Postmortem Casework
By George S. Behonick, Ph.D., F-ABFT, Laboratory Director, Chief Toxicologist
Synthetic compounds designed to mimic the pharmacology of various illegal drug classes infiltrated the illicit drug market during the last decade plus; this includes synthetic cannabinoids (“K2 Spice”), cathinones (“Bath Salts”), hallucinogens, and designer fentanyl analogs and opioids (examples such as fluorofentanyl, brophine and the nitazene compounds). In particular, the fentanyl analogs, along with illicitly manufactured fentanyl (IMF), imposed significant impact to the morbidity and mortality of drug-related exposures. Heroin cases experienced a dramatic resurgence around 2010; in large part, its unprecedented purity (users could ‘snort’ or insufflate the drug) and its relative low cost compared to prescription opioids (e.g. OxyContin®) fueled its unbridled demand as an alternative among opioid addicts and neophyte users. Gradually with time, solid dose materials (paraphernalia) and autopsy specimens began to demonstrate the concomitant presence of heroin and IMF. Ostensibly, the addition of IMF was designed to increase the potency of the product. Eventually, beginning in 2014 the proportion of IMF became greater than heroin in these mixtures. By 2015 the greater number of drug-involved cases included fentanyl, and not heroin. Simultaneous to this trend, numerous synthetic fentanyl analogs were being manufactured outside of the United States, but made available to illicit drug traffickers over the Internet. In 2016-17, carfentanil began appearing in seized solid dose drug products and medical examiner death investigation cases [5].
Carfentanil is a mu (µ) opioid receptor agonist; it is about 10,000 times more potent than morphine and demonstrates 30-100 times the potency of fentanyl [8]. Between September 1, 2016 and January 1, 2017, Axis Forensic Toxicology detected carfentanil in 262 postmortem blood specimens [6]. We described the specific details of 13 fatalities, from Indiana, Michigan, Kentucky and Ohio in this data set. Other investigators reported the detection of carfentanil in blood specimens obtained from impaired drivers and postmortem toxicology submissions [7, 4]. In response, state and federal agencies issued health alerts in 2018 which detailed the rising numbers of deaths involving fentanyl and fentanyl analogs to include carfentanil [2, 1].
2016 and 2017 demonstrated a surge increase in the number of drug-related deaths in the United Sates; that is, ↑11,228 (+21.4%) in 2016 and ↑6605 (+10.4%) in 2017; however, notably in 2018, drug-related deaths declined by 2,870 or -4.1%. The rise and fall coincided with increases, and then, decreases of carfentanil detections in seizure exhibits from 2015-2018. The overall availability of carfentanil was attributed to be a major factor in the accelerated, then diminished rate of drug-related deaths in the period 2016-2018 [3]. China banned carfentanil on March 1, 2017.
In CY 2022 Axis Forensic Toxicology detected carfentanil in two cases. Carfentanil was detected in one case in February 2023 however, in late spring and summer (May 26 – Aug 18), Axis Forensic Toxicology detected carfentanil in blood specimens from 9 postmortem cases. The time span being four months with the cases originating from four different states: Indiana (4), Wisconsin (2), Kentucky (2), and Ohio (1). A cursory review of a subset of these cases (n = 7) indicated 6 of 7 decedents to be male, with an age range of 29-61 years and median age of 41 years. Carfentanil postmortem blood concentrations exhibited a range of 47.2 to 409 picograms per milliliter (pg/mL); carfentanil was identified qualitatively in two of the cases. Multiple drugs were detected in all but one case. Fentanyl was detected in all cases with multiple drug detections. Methamphetamine and amphetamine was detected in 5 of the 7 cases. Other detections included: Acetylfentanyl (4 cases), 4-ANPP (4 cases), fluorofentanyl ( 1case) and morphine (1 case).
The aforementioned case accounts underscore the continued awareness and vigilance medico-legal death investigators and forensic toxicology laboratories must demonstrate to surveilling the drug carfentanil. In one case reported herein, the decedent, a 61 year old male, was found deceased in his vehicle at a truck stop that he was known to frequent on a near daily basis. The sole toxicological finding in this case was a carfentanil postmortem blood concentration of 403 pg/mL. In the two Wisconsin cases, the deaths occurred in two males who apparently knew each other and were suspected to have secured drugs from the same supplier within a close approximate time to each other. And in one Indiana case, investigators believed there was an association or a link to two other cases with respect to the source of the carfentanil. All three deaths occurred proximate to each other in time with a belief that the carfentanil supplier was one of the decedents. Detecting carfentanil in blood is a challenge because of the low (sub nanogram/mL or picogram/mL) presenting concentrations of the drug. Axis Forensic Toxicology presumptively screens for carfentanil in the Comprehensive panel (order code 70510) and the Indiana State Department of Health panel (test code 70575); this is accomplished by high resolution mass spectrometry ( Liquid Chromatography Quadrupole Time of Flight Mass Spectrometry) via the Analyte Assurance™ feature of the Comprehensive panel. Confirmation and quantitation of carfentanil is accomplished by LC-MS/MS (Liquid Chromatography Tandem Mass Spectrometry) in the Designer Opioids panel (order code 13810) with a carfentanil Lower Limit of Quantitation (LLOQ) of 10 pg/mL , or 0.010 ng/mL. Of note, carfentanil is not presumptively screened in the Drugs of Abuse panel (order code 70530), or in the customized Drugs of Abuse panel (Kentucky, order code 70555).
In summary, carfentanil exhibited a significant nationwide prevalence in postmortem cases in 2016-17; subsequent scheduling of the drug in the United States and a ban in China in 2017 resulted, in part, to a precipitous decline in positive postmortem cases. Axis Forensic Toxicology recognized a re-emergence of carfentanil in postmortem case work notably beginning the latter part of May 2023 and extending into August 2023 with a total of 9 detections from four states (IN, WI, KY and OH). Medico-legal death investigators, medical examiners, coroners and law enforcement agencies are urged to be alert to this observation. Death scene investigation, decedent social/drug history, autopsy and an appropriate scope of toxicology testing are of paramount importance in suspected drug-related cases. Drug intelligence trends in a given jurisdiction or region, as provided by local sources such as the Drug Enforcement Agency (DEA), law enforcement drug task forces together with information from state and federal drug testing laboratories are essential tools in identifying real time drug patterns in a specific location. Thus far in 2023, with the exception of 1 case from the total of 10, all of the carfentanil detections noted in the laboratory were punctuated by the parallel detections of IMF; likewise, methamphetamine and amphetamine was detected in 5 of the 7 cases reviewed as a subset to the ten case total observed thus far in 2023. Axis Forensic Toxicology will continue to monitor carfentanil case trends in the remainder of 2023.
Acknowledgements
The following individuals and jurisdictions are recognized for their contributions to this article by the provision of case investigative details, circumstances and decedent histories: Amy Lay, Medicolegal Death Investigator/Pathology Assistant, Lake County Coroner’s Office, IN; Steve Lockyear, Vanderburgh County, IN Coroner; Joe Hudson, Grayson County, KY Coroner; Josh Garvey, Iowa County, WI Deputy Coroner, and Dr. Robert F. Corliss, Professor and Autopsy Director-Department of Pathology and Laboratory Medicine, University of Wisconsin-Madison.
References
[1] Centers for Disease Control Health Update, CDCHAN-00413, Rising numbers of deaths involving fentanyl and fentanyl analogs, including carfentanil, and increased usage and mixing with non-opioids. July 11, 2018
[2] Delaware General Health District, Delaware County, Ohio Health Alert, Rising numbers of deaths involving fentanyl and fentanyl analogs, including carfentanil, and increased usage and mixing with non-opioids. July 12, 2018
[3] Jalal, H, Burke, DS. Carfentanil and the rise and fall of overdose deaths in the United States. Addiction. 2021 Jun; 116(6):1593-1599
[4] Papsun, D, Isenschmid, D, Logan, BK. Observed carfentail concentrations in 355 blood specimens from forensic investigations. J Analytical Tox. 2017; 41:777-778
[5] Schueler, HE. Emerging synthetic fentanyl analogs. Acad Forensic Path. 2017 7(1):36-40
[6] Shanks, KG, Behonick, GS. Detection of carfentanil by LC-MS-MS and reports of associated fatalities in the USA. J Analytical Tox. 2017; 41:466-472
[7] Tiscione, NB, Alford, I. Carfentanil in impaired driving cases and the importance of drug seizure data. J Analytical Tox. 2018; 42:476-484
[8] Wilde, M, Pichini, S, Pacifici, R, Tagliabracci, A, Paolo Busardo, F, Auwarter, V, Solimini, R. Metabolic pathways and potencies of new fentanyl analogs. Frontiers in Pharmacology. 2019 10:1-16
Read MoreNewly Scheduled Novel Psychoactive Substances
By Kevin Shanks, M.S., D-ABFT-FT
Novel psychoactive substances (NPS) are compounds designed or consumed to mimic the effects of typical recreational substances such as diacetylmorphine (heroin), cocaine, methamphetamine, cannabis, or even prescription medications. As these NPS emerge and become prevalent, the United States Federal government can use its scheduling powers to effectively ban the substances as Schedule I controlled substances.
Schedule I controlled substances are defined as a substance that has a high potential for abuse and no currently accepted medical use in the United States.
Effective July 26, 2023, the United States Federal government controlled the following NPS as Schedule I controlled substances: etizolam, flualprazolam, clonazolam, flubromazolam, and diclazepam. Over the past few years, each of these drugs have been associated with or implicated in numerous cases of driving under the influence of drugs as well as toxicity and fatality.
Axis tests for clonazolam, etizolam, flualprazolam, and flubromazolam in the Novel Psychoactive Substance panel (order code 13610) as well as the Comprehensive Panel with Analyte AssuranceTM (order code 70510). Diclazepam (as metabolites delorazepam and lorazepam) is also included in order code 70510. If you have questions about these substances and how they may apply to your casework, please reach out to our subject matter experts by email ([email protected]) or phone (317-759-4869, Option 3).
References
Department of Justice, Drug Enforcement Administration, 21 CFR Part 1309, Docket No. DEA-989. Federal Register. Volume 88, No. 142. Schedules of Controlled Substances: Temporary Placement of Etizolam, Flualprazola, Clonazolam, Flubromazola, and Diclazepam in Schedule I. July 26, 2023.
Read MoreA Closer Look at the Novel Emerging Compounds Panel: Alpha-PiHP and N,N-Dimethylpentylone
By Kevin Shanks, M.S., D-ABFT-FT
As mentioned in the previous post, novel psychoactive substances (NPS) come in different flavors – and opioids, cannabinoids, stimulants, hallucinogens, and benzodiazepines are just a few of them. The Novel Emerging Compounds (NEC) Panel offered by Axis Forensic Toxicology helps to detect the most newly emerged NPS on the drug market and is meant to continually evolve over time as new substances emerge on the street.
In the first post in this series, we took a look at two of the more recently emerged NPS benzodiazepines, and in this second post, we are looking at two of the most recently detected stimulants: alpha-PiHP and N,N-dimethylpentylone.
Alpha-PiHP, also known as 4-methyl-1-phenyl-2-(pyrrolidin-1-yl)pentan-1-one or alpha-pyrrolidinoisohexanophenone, is a substituted cathinone that is a positional isomer of the prescription medication pyrovalerone, a norepinephrine-dopamine reuptake inhibiting drug that is used for the treatment of chronic fatigue and as an appetite suppressant. Alpha-PiHP was first reported as being a drug sold on the illicit drug market in 2016 by the National Forensic Laboratory of Slovenia when it was detected in an off-white colored powder. In the United States in 2018, the Center for Forensic Science Research and Education (CFSRE) first reported the detection of the substance in a white solid material via the Department of Homeland Security.
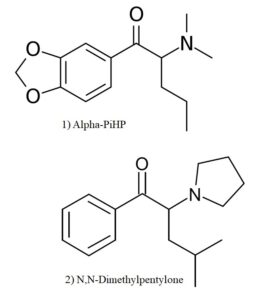
Chemical Structures of Alpha-PiHP, Dimethylpentylone Structures drawn by Kevin G. Shanks (2023).
N,N-dimethylpentylone is also known as 1-(1,3-benzodioxol-5-yl)-2-(dimethylamino)pentan-1-one or dipentylone and is a substituted cathinone that is a positional isomer of a previously reported cathinone, N-ethylpentylone, a norepinephrine-dopamine-serotonin reuptake inhibitor. Pentylone is a common metabolite produced by the body via de-ethylation after consumption of N,N-dimethylpentylone. The drug was first identified in Sweden in 2014, but didn’t emerge in the United States until 2021-2022.
Similar to other classical stimulants such as methamphetamine and amphetamine, these two compounds act pharmacologically as central nervous system stimulants with activity involving the neurotransmitters serotonin, norepinephrine, and dopamine. While the human pharmacology of these substances hasn’t been readily tested, it is surmised that they act as either direct releasers of the neurotransmitters or as transporter inhibitors. Reported effects after use of substances such as these include increased alertness, increased energy, euphoria, feelings of well-being, restlessness, and hallucination. Other physiological effects are hyperthermia, tachycardia, hypertension, mydriasis, diaphoresis, dehydration, and hyponatremia.
While not explicitly listed as controlled substances in the United States, both of the substances may be considered positional isomers of already controlled drugs and therefore be considered “analogues”. According to the Drug Enforcement Administration’s (DEA) National Forensic Laboratory Laboratory Information System (NFLIS) 2022 Midyear Drug Report, N,N-dimethylpentylone was the third most common phenethylamine detected by the DEA – behind only methamphetamine and amphetamine. Alpha-PiHP was the sixth most commonly detected phenethylamine in 2022. Alpha-PiHP and N,N-dimethylpentylone have been implicated in human toxicity which have led to numerous hospitalizations and fatalities in the USA.
Axis qualitatively monitors both of these compounds in our NEC panel (order code 13710) and Comprehensive Panel, Blood with Analyte Assurance (order code 70510) using liquid chromatography with quadrupole time of flight mass spectrometry (LC-QToF-MS). Over the time range 01/30/2023 – 06/30/2023, Axis has detected alpha-PiHP in 11 blood specimens with all detections located in Florida and N,N-dimethylpentylone in 42 cases with 41 cases in Florida and 1 case in Indiana. The reason why these compounds have been predominately found in Florida is not known, but NPS and classical drug trends tend to be regional phenomena.
In Axis Forensic Toxicology casework, Alpha-PiHP was typically found alongside fentanyl/norfentanyl (n=6), 4-ANPP (n=5), N,N-dimethylpentylone (n=5), cocaine/benzoylecgonine (n=3), and naloxone (n=3). N,N-dimethylpentylone was simultaneously detected with fentanyl/norfentanyl (n=30), 4-ANPP (n=29), pentylone (n=21), cocaine/benzoylecgonine (n=18), and naloxone (n=14).
Axis also monitors other NPS stimulants in our Novel Psychoactive Substances panel (order code 13610). These additional compounds include alpha-PVP, butylone, dibutylone, dimethylone, eutylone, MDPV, mephedrone, methcathinone, methedrone, methylone, N-ethylpentylone, pentylone, and TFMPP. As always, if you have questions about these substances and how they may play a role in your medical-legal investigation, please reach out to our subject matter experts by email ([email protected]) or phone (317-759-4869, Option 3).
Stay tuned for the third post in the NEC Panel series! We will take a look at two more recently emerged novel compounds: phenibut and tianeptine.
Read MoreA Closer Look at the Novel Emerging Compounds Panel: Bromazolam and Flubromazepam
By Kevin Shanks, M.S., D-ABFT-FT
Novel psychoactive substances (NPS) come in different varieties – opioids, cannabinoids, stimulants, hallucinogens, and benzodiazepines are just a few of the families on the illicit drug market. Axis developed the Novel Emerging Compounds (NEC) Panel to help detect the most newly emerged NPS on the drug market. The panel is meant to continually evolve in scope as new substances emerge on the street and then either continue to be prevalent or possibly disappear from the market.
This is intended to be a series of multiple posts briefly describing the compounds in the current iteration of the NEC Panel.
In the recent past, we have seen the emergence of NPS benzodiazepines such as etizolam, clonazolam, and flualprazolam. In this first summary of the NEC Panel, we are looking at two of the more recently emerged compounds are bromazolam and flubromazepam.
Bromazolam is a drug that has a history in pharmaceutical drug development as it was first synthesized in the 1970s as XLI-268, but it was never approved for medicinal use. The first emergence of bromazolam on the illicit drug market in the United States was in 2019, but it never became prevalent until more recently. The substance is the brominated analog of alprazolam, meaning it has a bromine atom in the place of the typical chlorine atom.
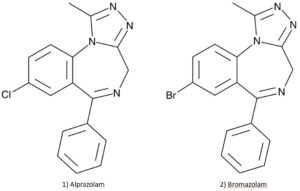
Chemical Structure Comparison of Alprazolam and Bromazolam Structures drawn by Kevin G. Shanks (2023).
Flubromazepam is a drug that also has a history in pharmaceutical drug development. It was first synthesized in 1960, but it did not receive any further study as a medicine. It appeared on the illicit drug market in 2012, but didn’t gain any traction for several years. Flubromazepam is a fluorinated analog of phenazepam, a benzodiazepine used as a medicine in Russia, meaning it has a fluorine atom in the place of the typical chlorine atom.
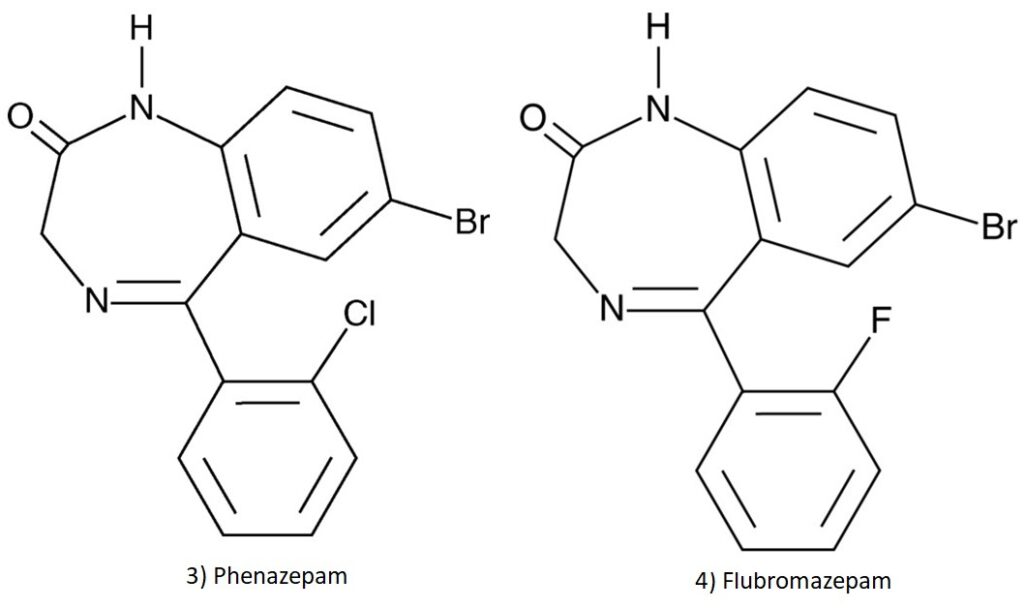
Chemical Structure Comparison of Phenazepam and Flubromazepam. Structures drawn by Kevin G. Shanks (2023).
Similar to other classical benzodiazepines such as alprazolam (Xanax), diazepam (Valium), or clonazepam (Klonopin), these compounds act pharmacologically as GABA (gamma-amino butyric acid) receptor agonists. They bind to the GABA receptor and initiate a change in chloride ion channels which leads to inhibition in the central nervous system. Common adverse effects reported by users of NPS benzodiazepines are consistent with those reported after using the classical benzodiazepines and include drowsiness, tiredness, sedation, loss of motor coordination, slurred speech, amnesia, and respiratory depression. Both bromazolam and flubromazepam are not considered controlled substances by the United States Federal government, but may be controlled at a state level as Schedule I controlled substances. Data from the Drug Enforcement Administration’s (DEA) National Forensic Laboratory Information System in 2022 showed that bromazolam was now in the top 15 reported tranquilizers and depressants in the United States. Both bromazolam and flubromazepam have been previously implicated in human intoxication cases involving driving motor vehicles as well as being involved in toxicity leading to fatality.
Axis qualitatively monitors both of these compounds in our NEC panel (order code 13710) and Comprehensive Panel, Blood with Analyte Assurance (order code 70510) using liquid chromatography with quadrupole time of flight mass spectrometry (LC-QToF-MS). Over the time range 01/30/2023 – 06/30/2023, Axis has detected flubromazepam in 3 blood specimens across 3 states (Indiana, Ohio, and South Dakota) and bromazolam in 72 blood specimens across 15 states (California, Colorado, Florida, Indiana, Iowa, Kansas, Kentucky, Louisiana, Michigan, Missouri, Nebraska, Ohio, Tennessee, Texas, and Wisconsin). Bromazolam was commonly detected alongside fentanyl/norfentanyl (n=59), 4-ANPP (n=46), acetylfentanyl (n=27), THC/THC-COOH (n=21), methamphetamine (n=20), and cocaine/benzoylecgonine (n=19). Flubromazepam was typically detected alongside gabapentin/pregabalin (n=3) and fentanyl (n=2).
Axis also monitors other NPS benzodiazepines in our Novel Psychoactive Substances panel (order code 13610). These additional compounds include adinazolam, clonazolam, etizolam, flualprazolam, and flubromazolam. As always, if you have questions about these substances and how they may apply to your toxicology casework or investigation, please reach out to our subject matter experts by email ([email protected]) or phone (317-759-4869, Option 3).
Stay tuned for the second post in the NEC Panel series – where we will take a look at two of the more recently emerged stimulant compounds: alpha-PiHP and N,N-dimethylpentylone.
Read MoreCannabinoids Panel Update
Dear Valued Client,
In the spirit of continuous improvement, to provide the most relevant panels and tests in the industry, our products are periodically updated to provide new and relevant offerings. It is with that goal in mind that we announce an update to our 44050: Cannabinoids, Blood Order Code. This panel, and likewise the 70510: Comprehensive Panel with Analyte Assurance and 70530: Drugs of Abuse Panel, will include Delta-8 THC and 11-Hydroxy Delta-9 THC beginning with orders placed on or after July 17th, 2023. You can always find the most recent publication for our panel offerings on our Test Catalog, found at www.axisfortox.com.
The cannabis industry continues to grow and with it, new challenges arise as laws and regulations change surrounding it. One such challenge is the rise of different cannabinoid isomers being sold to try and circumvent these laws. Delta-8-THC, pictured below beside delta-9-THC, is one such isomer that has gained attention.
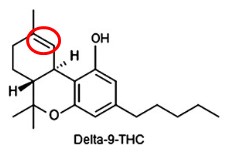
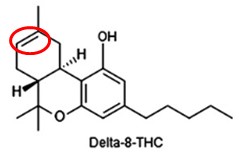
The claim of manufacturers and sellers is that the isomer exists in a legal gray area due to the 2018 Farm Bill. We are toxicologists, not lawyers or lawmakers, so we cannot give our opinion on whether this is correct or not. No matter what is decided, the compound is being widely sold and may be relevant to your casework and we can help with the toxicology of that.
Delta-8-THC is very similar to delta-9-THC which is considered the primary component in cannabis products. Its potency is less than that of delta-9-THC but has a similar psychoactive effect. The metabolism of each produces an 11-hydroxy-THC metabolite which is an active metabolite. This is further metabolized into a carboxylic acid metabolite, 11-nor-9-carboxy-THC.
The cannabinoids that occur naturally are not going to typically be contributing directly to cause of death. The presence of such substances may indicate that the individual was under the influence but toxicology testing alone cannot be used to determine if an individual was under the influence. Toxicology results must be paired with the scene investigation and witness statements to make this determination.
If you have any questions regarding these new analytes and application to your casework, please reach out to us via email at [email protected] or via phone at 317-759-4869 option 3.
Read MoreXylazine Presentation at MATT Conference 2023
By Stuart Kurtz, D-ABFT-FT
In April, I spoke at the Midwest Association of Toxicology and Therapeutic Drug Monitoring (MATT) annual conference in Columbus, OH. The title of the talk was “Detection of Xylazine in Postmortem Specimens With Fentanyl, Morphine, Methamphetamine, and Cocaine From 2021-2022.” The conference was a great opportunity to talk shop with peers from the Midwest region and hear what they are doing. In this post, I will summarize what was presented at the MATT conference.
Xylazine was first synthesized as an antihypertensive by Bayer in 1962. During clinical trials, it was found to have additional central nervous system (CNS) depression effects. Despite being investigated for use as an antihypertensive agent, some patients would initially experience hypertension before the desired effect of a reduction of blood pressure. Some patients also experienced much more severe hypotension than intended. Due to these findings, it was rejected for human medical use and only approved for veterinary purposes.
A survey done by Texas Poison Control looked at the reported effects of xylazine toxicity. The major reported adverse effects were drowsiness and lethargy (47%), bradycardia (20%), hypotension (11%), hypertension (9%), and slurred speech (8%). Analgesic effects have been reported but the mechanism is not well understood, and the effect is minimal compared to its other adverse effects. There are two theories behind the mechanism. One immunoassay study found that xylazine could weakly displace opioids at binding sites. In this study, naloxone was not seen to reverse the effects. The other theory is that xylazine stimulates the release of endogenous opioids which could be reversed by naloxone. These are theories that have been reported but further study is needed.
Published case reports involving xylazine typically describe the presence of at least one other additional substance in combination with xylazine which may lead to an additive effect. When xylazine is the primary substance of toxicological interest detected in casework, there is a competing cause of death or an intentional overdose as determined by the scene investigation. The blood concentration range in these cases was 2,300-11,000 ng/mL. In cases of intentional overdose, the decedents worked in the veterinary field and had access to xylazine. The case involving a xylazine blood concentration equal to 2,300 ng/mL was ruled suicide by hanging after injection of xylazine. One attempted suicide case had a serum concentration of 4,600 ng/mL with the individual making a recovery with medical intervention. Two other fatal cases involving xylazine had blood concentrations of xylazine (200 ng/mL)/nordiazepam (2,500 ng/mL)/ and xylazine (300 ng/mL)/flualprazolam (1,100 ng/mL). In driving under the influence of drugs (DUID) casework, a range of 5.1-450 ng/mL of xylazine in blood was found. Full case histories were not available so it is unknown if any of those individuals died from effects of xylazine with other drugs that may have been present. A case of 570 ng/mL in blood was reported from a driver who passed out in their car but could be awakened.
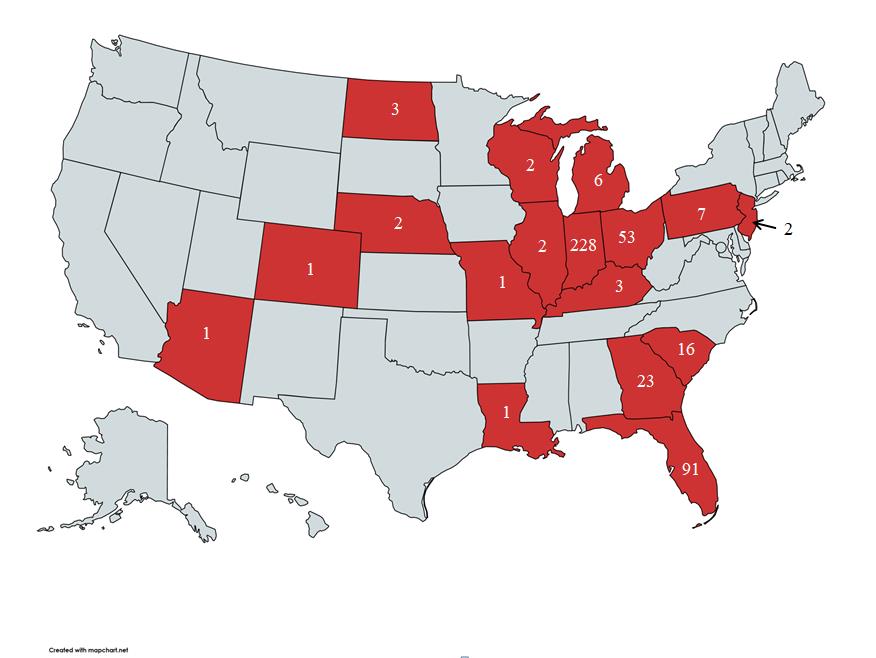
A heat map of xylazine detections based on data from Axis Forensic Toxicology’s lab.
For the years 2021-2022, we had 442 total detections of xylazine. For reference, we receive about 22,000-24,000 cases per year. The following drugs were commonly detected alongside xylazine: fentanyl (92%), benzoylecgonine (29%), methamphetamine (26%), morphine (12%). In 26% of the cases, the combination of xylazine, fentanyl, and methamphetamine was observed, while in 4% of the cases, the combination of xylazine, fentanyl, methamphetamine, and benzoylecgonine was detected.
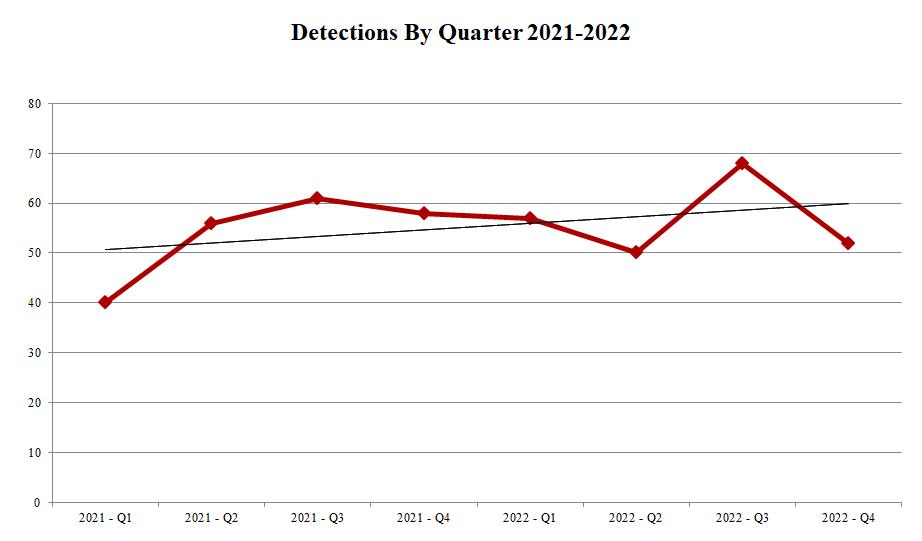
Xylazine detections by quarter have risen slightly since Q1 2021.
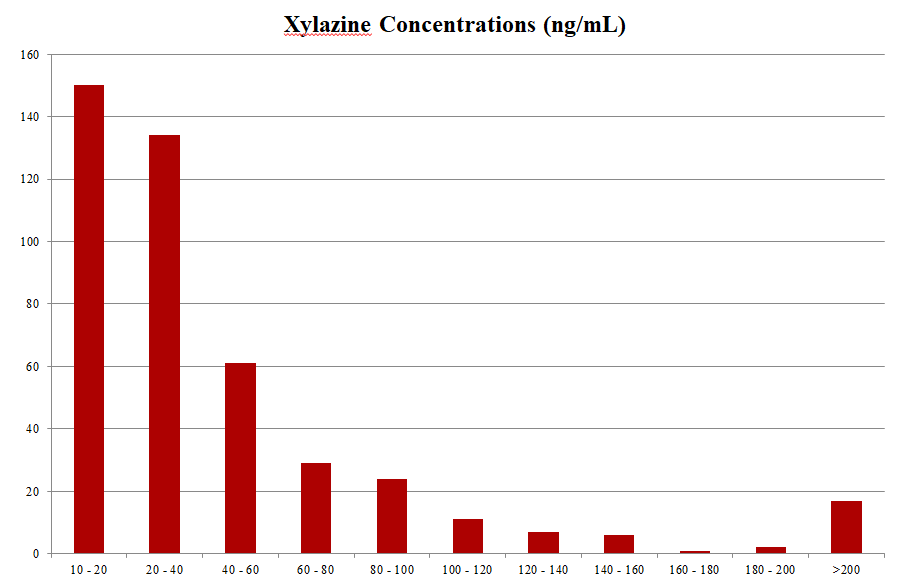
64% of xylazine detections fall in the concentration range of 10-40 ng/mL.
Because of the lack of data surrounding human clinical use of xylazine and the lack of reports of sole xylazine use, it is hard to determine what postmortem blood concentrations could be considered fatal. Xylazine is almost always found in combination with another drug due to its popular use as an adulterant. Its CNS depression effects can mimic other compounds such opioids and benzodiazepines and it is not scheduled as a controlled substance by the Drug Enforcement Administration (DEA) in the United States, so access is not very restricted. Because of its additive effects with other CNS depressants, it can still be relevant in postmortem toxicology, and it is included in our comprehensive panel of testing.
Wounds associated with xylazine use have been reported in Philadelphia, PA. We have not received any reports of wounds potentially associated with xylazine use. Also, in talking with other forensic toxicologists around the country, we have not heard from them any other reports of these wounds being present in their locations.
As always, please reach out to us if you have any questions about this post. We can be emailed at [email protected] or you can call us at 317-759-4869 option 3.
Sherri L Kacinko, Amanda L A Mohr, Barry K Logan, Edward J Barbieri, Xylazine: Pharmacology Review and Prevalence and Drug Combinations in Forensic Toxicology Casework, Journal of Analytical Toxicology, Volume 46, Issue 8, October 2022, Pages 911–917, https://doi.org/10.1093/jat/bkac049
Karla A. Moore, Mary G. Ripple, Saffia Sakinedzad, Barry Levine, David R. Fowler, Tissue Distribution of Xylazine in a Suicide by Hanging, Journal of Analytical Toxicology, Volume 27, Issue 2, March 2003, Pages 110–112, https://doi.org/10.1093/jat/27.2.110
Malayala SV, Papudesi BN, Bobb R, Wimbush A. Xylazine-Induced Skin Ulcers in a Person Who Injects Drugs in Philadelphia, Pennsylvania, USA. Cureus. 2022 Aug 19;14(8):e28160. doi: 10.7759/cureus.28160. PMID: 36148197; PMCID: PMC9482722.
Way Koon, Teoh & Muslim, Noor & Chang, Kah Haw & Abdullah, Ahmad Fahmi Lim. (2022). Abuse of Xylazine by Human and its Emerging Problems: A Review from Forensic Perspective. Malaysian Journal of Medicine and Health Sciences. 18. 190-201. 10.47836//mjmhs18.4.26.
Read MoreVitreous Chemistries, part 2.
By Stuart Kurtz, M.S. D-ABFT-FT
As discussed in the previous blog post, vitreous humor has many caveats when interpreting its results in the context of postmortem toxicology. For those considerations and some background on vitreous humor, check out that post first (https://axisfortox.com/vitreous-chemistries-pt1).
Vitreous humor can be used in instances where a drug or dug metabolite is quickly eliminated from the blood and it is known to cross into the vitreous and be detectable. One such metabolite is 6-acetylmorphine (6-AM) which is a marker for heroin exposure. Heroin is not typically looked for in blood samples because of its extremely short half-life at around 5-10 minutes. It metabolizes into 6-AM, which has a longer half-life at around 30 minutes, but it still may not be detectable in blood. Once 6-AM metabolizes into morphine, it is impossible to determine pharmaceutical morphine vs. heroin as the source. Urine would be the best matrix to look for the presence of 6-AM but vitreous humor is also a good option if urine isn’t available.
Electrolytes testing is one of the most common uses for vitreous humor. This usually includes sodium, potassium, chloride, glucose, urea nitrogen, and creatinine. Sodium and chloride concentrations in vitreous will approximate serum concentrations. Potassium concentrations will rapidly increase postmortem. Urea nitrogen and creatinine are similar to sodium and chloride in terms of correlation with serum concentrations and can be used as indicators for dehydration. Glucose concentrations in vitreous are more reliable than blood glucose concentrations prior to death. However, glucose vitreous concentrations dissipate rapidly in the postmortem interval. Therefore, although a diagnosis of hyperglycemia may be made from elevated vitreous glucose concentrations, a diagnosis of hypoglycemia cannot be made because of the time rate disappearance of glucose from the matrix. Postmortem blood glucose concentrations are considered unreliable and vitreous should be used when possible.
The significance of vitreous glucose is in helping to determine if diabetes played a part in cause of death. Elevated vitreous glucose is a good indicator that someone was experiencing a diabetic event. This can often be corroborated with acetone presence in the blood and/or vitreous humor. Additional testing for beta-hydroxybutyrate (BHB) can be done in blood if a diabetic event is suspected. Diabetes tends to not have any signs at autopsy so blood and vitreous testing can be helpful. BHB is the primary ketone that is produced during ketoacidosis. Diabetic ketoacidosis is typically associated with elevated glucose in vitreous humor. Medical history can also be very important if vitreous volume is limited or unobtainable.
The presence of acetone and normal glucose can be an indicator of some other form of ketoacidosis. Alcoholic ketoacidosis may occur in cases of binge drinking alcoholic beverages. As is typical with chronic alcoholism, the person will have evidence of liver disease. The underlying cause is malnourishment which can also occur independently of alcoholism. Malnourishment may also be associated with dehydration which would be indicated by elevated urea nitrogen, sodium, and chloride concentrations. Ultimately, diabetic vs. alcoholic vs. malnourishment ketoacidosis requires additional information beyond just the toxicology testing.
Medical history and an autopsy are very important for contextualizing the results we can provide for you in these cases. If your case potentially involves dehydration, it may be prudent to check the vitreous for sodium, potassium, or chloride, whereas if your case involves potential issues with diabetes or diabetic ketoacidosis, it would be necessary to order testing for vitreous chemistries to include glucose. If kidney function is a potential area of concern, evaluation of urea nitrogen and creatinine would be important. Again, as always in forensic toxicology, case circumstances and underlying pathology will aid in determining the best course of action when considering vitreous humor chemistry and electrolytes testing.
Please reach out to us if you have any questions regarding this topic or want help with deciding what testing may be necessary. Our email is [email protected] and our phone number is 317-759-4869 option 3.
References
Guidelines for the Interpretation of Analytical Toxicology Results. Disposition of Toxic Drugs and Chemicals in Man. Twelfth Edition. Randall C. Baselt. Biomedical Publications. Pages xxx-xlii. (2020).
Introduction to Forensic Toxicology. Clarke’s Analytical Forensic Toxicology. Sue Jickells and Adam Negrusz. Pharmaceutical Press. Pages 1-12. (2008).
Postmortem Toxicology. Clarke’s Analytical Forensic Toxicology. Sue Jickells and Adam Negrusz. Pharmaceutical Press. Pages 191-218. (2008).
Postmortem Forensic Toxicology. Principles of Forensic Toxicology. Fourth Edition. Barry Levine. AACC, Inc. Pages 3-14. (2017).
Read MoreVitreous Chemistries, part 1.
By Stuart Kurtz, M.S. D-ABFT-FT
The purpose of these next two blog posts is to discuss the utility that vitreous humor provides in the context of a case. This first post will focus on what vitreous humor is and the caveats associated with its interpretation. The second post will discuss some scenarios in which it can be very useful.
Vitreous humor is the fluid found in the eyes between the lens and retina. There is approximately 2 mL of fluid in each eye meaning the volume is limited for testing. Because of this, we don’t recommend the use of vitreous humor as the primary specimen, and we do recommend careful consideration before attempting testing on it. The context of the case is always important and sometimes that is the most useful sample to test. Therefore, from a whole case investigation approach, we recommend always collecting vitreous humor, alongside blood and/or urine, at autopsy – if possible. Collection should be done in a tube without sodium fluoride or potassium oxalate as a preservative. The clear top tubes that are provided in our toxicology kits are well suited for vitreous collection, having no preservatives.
The primary components of vitreous humor are a connective tissue gel and transparent liquid that is primarily water. Its composition and location mean that it is quite stable and resistant to putrefactive changes postmortem. Movement of substances in and out of the vitreous happens by diffusion, osmotic pressure, convection, or active transport. Low molecular weight substances, such as ethanol, acetone, methanol and isopropanol, will travel in and out via diffusion. Most drugs that are important in postmortem testing are a much higher molecular weight and will travel in and out via convection.
Ultimately, the mechanisms for most substances entering the vitreous are mostly unknown and/or not well studied. Drugs such as fentanyl, methamphetamine, and cocaine might be found in vitreous humor but the ability to correlate to a blood concentration is extremely limited and not recommended. Most drugs are very fat soluble and the vitreous humor is mostly water. So just like with oil and water, drugs will not be easily dissolved in the small volume present.
Whereas with urine we expect that the majority of drugs will be found there in one form at some point post-exposure, that may not be the case with vitreous humor. There may be some drugs that are so poor in their ability to enter the vitreous humor that they would be undetectable. It can have some ability to show recent exposure, similar to urine, of a drug, but the absence of a drug should be interpreted with caution.
Our next post will discuss vitreous humor’s important use in forensic toxicology. As always, we are here to assist you. Please reach out to us if you have any questions regarding this topic or want help with deciding what testing may be necessary. Our email is [email protected] and our phone number is 317-759-4869 option 3.
References
Guidelines for the Interpretation of Analytical Toxicology Results. Disposition of Toxic Drugs and Chemicals in Man. Twelfth Edition. Randall C. Baselt. Biomedical Publications. Pages xxx-xlii. (2020).
Introduction to Forensic Toxicology. Clarke’s Analytical Forensic Toxicology. Sue Jickells and Adam Negrusz. Pharmaceutical Press. Pages 1-12. (2008).
Postmortem Toxicology. Clarke’s Analytical Forensic Toxicology. Sue Jickells and Adam Negrusz. Pharmaceutical Press. Pages 191-218. (2008).
Postmortem Forensic Toxicology. Principles of Forensic Toxicology. Fourth Edition. Barry Levine. AACC, Inc. Pages 3-14. (2017).
Read MoreAxis – Experts on Xylazine
By Denise Purdie Andrews
Recent industry news has been consumed with xylazine as the latest drug adulterant on the streets. Axis, your leading toxicology partner, has been testing for xylazine for several years and is prepared to assist you with questions about it and its effects. Testing for xylazine is included as a confirmed analyte in our 70510 Comprehensive Panel with Analyte Assurance™. While xylazine has been in the news lately, its importance as an adulterant should not overshadow the danger posed by fentanyl and other primary drugs of abuse.
This month, Stuart Kurtz, one of Axis’ expert toxicologists, will be speaking about xylazine with other toxicologists at the Midwest Association for Toxicology & Therapeutic Drug Monitoring Conference. This upholds Axis’ commitment to sharing its expertise with stakeholders within its industry and related communities. As the news reports, Xylazine detections alongside commonly seen drugs have risen in recent years. It was never approved for use in humans so its exact effects on the human body are not well understood. This talk takes a look at the data Axis has collected over the last 2 years of testing. Specifically, we looked at its detection with fentanyl, morphine, methamphetamine, and cocaine. While postmortem toxicology testing cannot determine if a specific combination of drugs was taken by an individual, it can be used to help guide public health policies. We will be sharing more information about the content of this presentation later in the month.
Please also join us in congratulating Stuart on becoming Axis’ newest ABFT-certified toxicologist!
Read More