BLOG & STORIES
Axis Adds Analytes to our Comprehensive Panel with Analyte Assurance™
We’re pleased to inform you that our Comprehensive Panel with Analyte Assurance™, along with the referenced panels below, will be updated for all orders effective September 29, 2025. The following analytes will be added:
- 5F-ADB Butanoic Acid Metabolite – Confirmed via Synthetic Cannabinoids Panel
- 7-Hydroxymitragynine – Confirmed via Novel Emerging Compounds Panel
- MDPHP – Confirmed via Novel Emerging Compounds Panel
- BTMPS – Confirmed via Novel Emerging Compounds Panel
- Diphenidine – Confirmed via Novel Emerging Compounds Panel
As with all components of Analyte Assurance™, if any of these analytes screen positive, our Lab Client Support team will contact you directly to determine whether confirmatory testing is desired.
At Axis Forensic Toxicology, we are committed to evolving with the needs of our clients and the ever-changing landscape of emerging substances. These additions reflect our proactive approach to ensuring you receive the most comprehensive and reliable testing services available.
If you have any questions or would like more information regarding this update, please don’t hesitate to reach out to us at [email protected]. Our team is always ready to assist.
Thank you for your continued partnership and trust in Axis. We look forward to continuing to support your work with the highest quality service and testing solutions.
Sincerely,
Matt Zollman
Director of Operations & Product Management
The Utility of Drug Testing in Urine
By Laureen Marinetti, PhD, F-ABFT
As part of its whole case approach, Axis Forensic Toxicology includes urine drug testing alongside blood testing in both the Comprehensive Panel with Analyte Assurance™ and Drugs of Abuse Panel. The standard urine screen typically covers common drugs of abuse, excluding barbiturates and cannabinoids—though these can be added upon request.
Urine often contains higher concentrations of drugs and metabolites than blood, and substances may remain detectable in urine for days or longer after use.
 Drug-Facilitated Crime Committee. PowerPoint DFSA, DFCC 2017")
From The Society of Forensic Toxicologists (SOFT) Drug-Facilitated Crime Committee. PowerPoint DFSA, DFCC 2017
The primary value of urine drug findings lies in their ability to reveal past drug use. Historical drug use may or may not be relevant to a case. For instance, blood results may show no detectable levels of stimulants such as cocaine or methamphetamine, while urine results are positive—indicating prior use. This information could be significant if the decedent had underlying cardiac disease.
In another scenario, urine results may suggest illicit drug use even when blood results are negative. This can help establish a timeline of drug use or corroborate blood findings. However, the concentration of drugs in urine is generally not useful for determining prior blood levels or the timing of drug use.
Quantitative urine values are only meaningful in specific contexts—such as when extensive comparative data to blood exists (e.g., ethanol), or when distinguishing endogenous from exogenous exposure (e.g., GHB). Axis provides urine concentration data only when it offers interpretive value.
In summary, Axis Forensic Toxicology incorporates urine drug testing alongside blood analysis to provide a more complete picture in forensic investigations. Urine testing is particularly valuable for detecting past drug use, as many substances remain in urine longer and at higher concentrations than in blood. While urine results cannot determine the timing or quantity of drug use, they can offer critical context—especially in cases involving underlying health conditions or suspected substance abuse. Quantitative urine data is only reported when it has clear interpretive value. As always, please do not hesitate to contact Axis Forensic Toxicology with any questions, concerns, or for assistance with case interpretation. Our team is committed to supporting your investigative needs with accurate and insightful toxicological analysis and interpretation.
Read More4-ANPP in Biological vs. Non-Biological Samples: The Interpretation is not the Same
By Kevin Shanks, M.S., D-ABFT-FT
We have previously discussed both fentanyl and 4-ANPP in this blog (1-2), but briefly, fentanyl is a mu opioid receptor agonist that is used as both a pharmaceutical medication and as an illicit drug found on the street typically as a powder or tablet. Fentanyl itself is metabolized primarily by the CYP3A4 enzyme in the human body. It can be dealkylated, hydroxylated, methylated, and hydrolyzed (3-4). At Axis, we monitor for the presence of the unchanged drug, fentanyl, alongside its primary metabolite, norfentanyl, in blood and urine. Several years ago, we added a second fentanyl-related substance to the scope of testing – 4-ANPP.
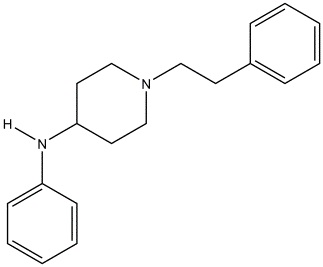
Chemical structure of 4-ANPP
Drawn by Kevin G. Shanks (2022)
So, what is 4-ANPP? The substance is known chemically as N-phenyl-1-(2-phenylethyl)-4-piperidinamine, but is also referred to as despropionyl fentanyl. It is formed via amide hydrolysis of the parent substance. It is considered to be a minor inactive metabolite of fentanyl – meaning it does not produce a pharmacological effect on the body (5-6). But it is also a precursor or starting material used in the synthesis of illicitly manufactured fentanyl and various related fentanyl derivatives or analogs. As an example, 4-ANPP can be reacted with propionyl anhydride to form fentanyl or acetic anhydride to form acetylfentanyl. 4-ANPP is not used in the synthesis of pharmaceutical-grade fentanyl.
Why is all of this important? The presence of illicitly manufactured fentanyl in the street drug supply in the USA has rapidly increased over the past 10-12 years (7). And with that increased presence comes a large increase in overdose deaths due to the substance. Recent CDC data shows that over 100,000 people died yearly from drug overdoses in the USA in 2022-2024, with the major driving factor being the prevalence of illicit fentanyl in the street drug supply (8).
Ultimately, the presence of 4-ANPP in a biological specimen such as blood or urine is merely a marker for fentanyl use or exposure. The product used may have been either pharmaceutical fentanyl or illicitly manufactured fentanyl. The origin of the fentanyl – pharmaceutical vs. street – cannot be determined by the toxicology results alone. In order to ascertain if 4-ANPP is present in the body from metabolism or if it was ingested by using an impure illicit street product, testing must be conducted on evidence from the scene which may include unidentified powders or tablets. If 4-ANPP is detected in the non-biological evidence, then it may be determined that the fentanyl exposure is from a non-pharmaceutical origin.
Axis Forensic Toxicology tests for the presence of 4-ANPP in our Comprehensive Drug Panel with Analyte Assurance™, Blood (order code 70510), which is completed by liquid chromatography with quadrupole time of flight mass spectrometry (LC-QToF-MS) and liquid chromatography with tandem mass spectrometry (LC-MS/MS). The reporting limit is 100 pg/mL and the substance is reported as qualitatively positive or negative – it is not reported quantitatively.
If you have any questions regarding the presence or absence of 4-ANPP or its role in your toxicology casework, please reach out to Axis’ subject matter experts at [email protected].
References
- Drug Primer: Fentanyl (2021). Axis Forensic Toxicology Blog. Drug Primer: Fentanyl – Axis Forensic Toxicology (axisfortox.com).
- Drug Primer: 4-ANPP (2022). Axis Forensic Toxicology Blog. Drug Primer: 4-ANPP – Axis Forensic Toxicology (axisfortox.com).
- Fentanyl. Disposition of Toxic Drugs and Chemicals in Man. Twelfth Edition. Randall C. Baselt. Biomedical Publications. Pages 844-847. (2020).
- Opioids. Principles of Forensic Toxicology. Fourth Edition. Barry Levine. AACC, Inc. Pages 271-291 (2017).
- Labroo, R.B., Paine, M.F., Thummel, K.E., Kharasch, E.D. (1997) Fentanyl Metabolism by Human Hepatic and Intestinal Cytochrome P450 3A4: Implications for Interindividual Variability in Disposition, Efficacy, and Drug Interactions. Drug Metabolism and Disposition, 25: 9. 1072-1080.
- Wilde, M., Pichini, S., Pacifici, R., Tagliabracci, A. et al. (2019) Metabolic Pathways and Potencies of New Fentanyl Analogs. Frontiers in Pharmacology, 10: 238. 1-16.
- 2022 Annual Drug Report. National Forensic Laboratory Information System (NFLIS). Drug Enforcement Administration. Springfield, VA.
- Provisional Drug Overdose Death Counts. National Vital Statistics System. Center for Disease Control. Vital Statistics Rapid Release – Provisional Drug Overdose Data. (Accessed 07/31/2025).
About the Newest Stimulants: N-Isopropyl Butylone and N-Cyclohexyl Methylone
By Kevin Shanks, M.S., D-ABFT-FT
As mentioned in several previous posts on this blog, novel psychoactive substances (NPS) are arranged into different families. Opioids, cannabinoids, stimulants, hallucinogens, and benzodiazepines are the main ones we encounter in forensic toxicology. Axis makes an effort to be able to detect the most newly emerged of these NPS as the drug market evolves over time. In this post, we will take a brief look at two stimulants which have recently appeared in the United States.
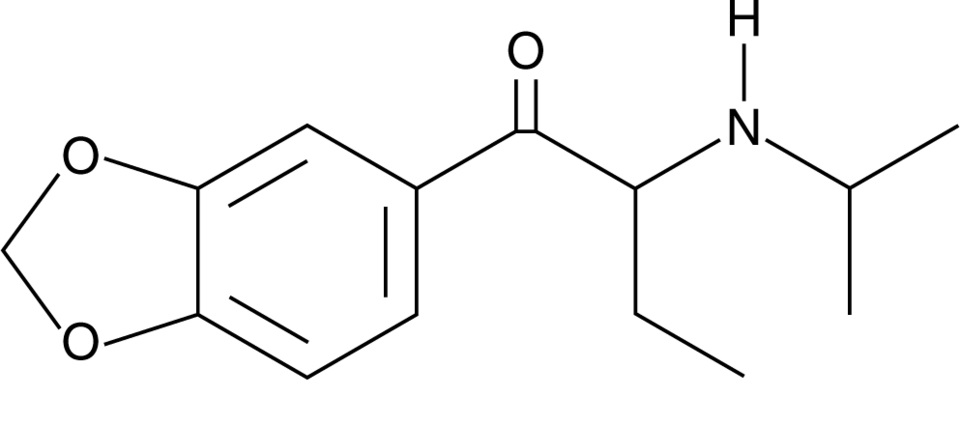
Chemical structure of N-isopropyl butylone Drawn by Kevin G. Shanks (2025)
N-isopropyl butylone and N-cyclohexyl methylone are considered substituted cathinones, which are a class of compounds related to cathinone, a naturally occurring stimulant alkaloid found in the plant Catha edulis, also known as khat. Substituted cathinones are chemically and pharmacologically similar to amphetamine and methamphetamine and act as central nervous system stimulants. These compounds primarily act on monoamine transporters in the body and inhibit the reuptake of dopamine, norepinephrine, and/or serotonin and may also act as releasers of the same neurotransmitters. The result of this pharmacological action is an increased concentration of neurotransmitters in the nerve cell synapse, which leads to stimulant and empathogenic physiological effects on the body. Desired effects of stimulants include euphoria, increased energy, sociability, and alertness. Adverse effects include anxiety, agitation, paranoia, hallucinations, and aggression. Acute toxicity is manifested via hyperthermia, hypertension, and tachycardia, severe agitation, hallucinations, and potential seizure, rhabdomyolysis, kidney failure, and death. Chronic toxicity includes psychological dependence, cognitive impairment, sleep disorders, depression, and neurotoxicity within the dopaminergic and serotonergic neutrotransmitter systems.
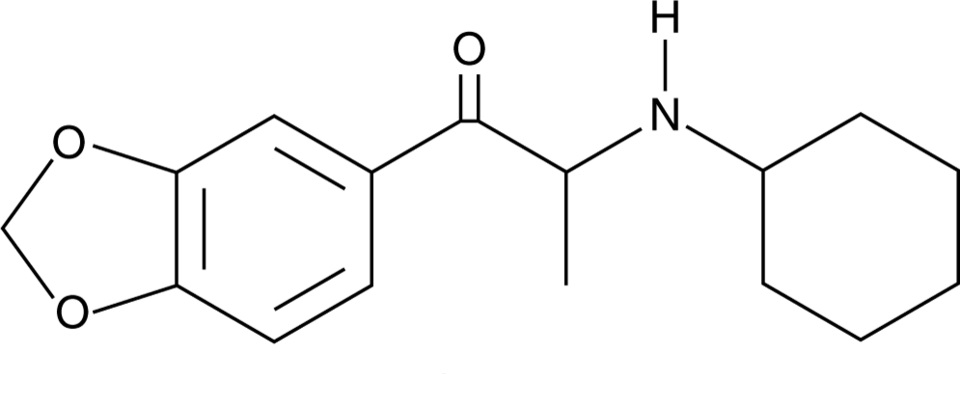
Chemical structure of N-cyclohexyl methylone Drawn by Kevin G. Shanks (2025)
N-isopropyl butylone was first identified in the United States in 2024 in the state of Georgia, where it was detected in drug material alongside methamphetamine. It was also detected in drug material sold as MDMA in New Zealand in 2024 and in drug material purported to be MDMA/ecstasy sold in Europe in 2025. In 2025, it was found alongside ketamine and methamphetamine. N-isopropyl butylone is a positional isomer of other substituted cathinones including N-ethylpentylone, N, N-dimethylpentylone, and N-propylbutylone.
N-cyclohexyl methylone was first identified in the United States in 2022 in drug material in the state of Florida when it was sold as an ecstasy tablet and in Indiana sold as a beige/off-white crystalline powder. The substance is a derivative of the older cathinone, methylone, which is itself a derivative of MDMA (3,4-methylenedioxymethamphetamine).
While not explicitly listed as controlled substances in the United States, both of the substances may be considered positional isomers of already controlled drugs and therefore be considered “analogues”. According to the Drug Enforcement Administration’s (DEA) National Forensic Laboratory Information System (NFLIS) March 2023 Drug Snapshot, N-cyclohexyl methylone was the third most common detected substituted cathinone in the United States with 257 reports. And in the December 2024 Drug Snapshot, N-isopropyl butylone was the most prevalent cathinone with 178 detections while N-cyclohexyl methylone was number 5 with 12 detections. There have not yet been any published reports of these two substances being implicated in human toxicity, including hospitalizations and fatalities.
Axis qualitatively monitors both compounds in our Novel Emerging Compounds (NEC) panel (order code 13710) and Comprehensive Panel, Blood with Analyte Assurance™ (order code 70510) using liquid chromatography with quadrupole time of flight mass spectrometry (LC-QToF-MS). Axis also monitors other NPS cathinones in the NEC panel including alpha-PHP, alpha-PiHP, and N, N-dimethylpentylone. Additional cathinone/stimulant compounds in our Novel Psychoactive Substances panel (order code 13610) include alpha-PVP, butylone, dibutylone, dimethylone, eutylone, MDPV, mephedrone, methcathinone, methedrone, methylone, N-ethylpentylone, pentylone, and TFMPP. As always, if you have questions about these substances and how they may play a role in your medical-legal investigation, please reach out to our subject matter experts by email ([email protected]) or phone (317-759-4869, Option 3).
Read MoreA New Fentanyl Derivative: ortho-Methylfentanyl
By Kevin Shanks, M.S., D-ABFT-FT
As we have discussed on this blog several times in the past, novel psychoactive substances (NPS) come in different varieties, which include cannabinoids, stimulants, opioids, benzodiazepines, and hallucinogens. One of Axis Forensic Toxicology’s objectives it to be able to detect the most recently emerged NPS on the street in a timely manner. With that said, a new fentanyl derivative has emerged!
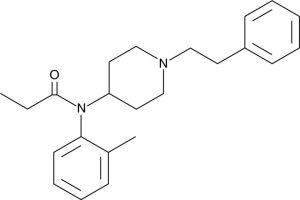
Chemical Structure of ortho-Methylfentanyl Drawn by Kevin G. Shanks (2025)
Ortho-Methylfentanyl is a fentanyl analog or derivative that has emerged in the United States as an NPS in both powders and counterfeit tablets. It has a chemical formula C23H30N2O and a molecular weight equal to 350.5 g/mol. It is structurally-related to fentanyl with the fundamental difference in chemical structure being in the position of a single methyl (-CH3) group, which is attached to the ortho- position of the phenyl ring. There are two other positional isomers: meta- and para-methylfentanyl. The ortho isomer of methylfentanyl was first detected in 2023 in British Columbia, Canada, but over the last two years, it was been detected across Canada and the United States. In the United States, the substance is considered a Schedule I controlled substance and is illegal to synthesize, possess, and distribute.
Pharmacologically, it is a mu (µ) opioid receptor agonist, much like morphine, oxycodone, and fentanyl. It also shares a similar analgesic potency with fentanyl. As a mu opioid receptor agonist, the effects of the substance would include analgesia, tiredness, drowsiness, sedation, and in overdose, severe respiratory depression, hypoxia, apnea, coma, and potentially, death.
In early 2025, we first detected ortho-methylfentanyl in our postmortem toxicology sample population and have now added it to our Designer Opioids panel (order code 13810) and the Comprehensive Panel, Blood with Analyte Assurance™ (order code 70510) using liquid chromatography with quadrupole time of flight mass spectrometry (LC-QToF-MS). Reporting limit is 50 pg/mL.
Axis also has the ability to monitor other novel opioids to include acetylfentanyl, acrylfentanyl, AP-237, AP-238, betahydroxythiofentanil, brorphine, carfentanil, cis-3-methylfentanyl, cyclopropylfentanyl, furanylfentanyl, isobutrylfentanyl, methoxyacetylfentanyl, ocfentanil, para-fluorobutyrylfentanyl, para-fluoroisobutyrylfentanyl, tetrahydrofuranfentanyl, tianeptine, U-47700, and valerylfentanyl.
As always, if you have questions about ortho-methylfentanyl and how it (or any other novel emerging compound) may play a role in your medical-legal investigation, please reach out to our subject matter experts by email ([email protected]) or phone (317-759-4869, Option 3).
Stay tuned to this blog for more quick drug primers on more novel compounds we have recently added to our testing scope!
Read MoreAxis Adds Analytes to our Comprehensive Panel with Analyte Assurance™
We’re excited to share that our Comprehensive Panel with Analyte Assurance™, as well as the below referenced panels, have been updated in all orders effective June 2nd, 2025. The analytes that have been added are as follows:
- ortho-Methylfentanyl – Confirmed via Designer Opioids Panel
- N-Cyclohexyl Methylone – Confirmed via Novel Psychoactive Substances Panel
- N-Isopropyl Butylone – Confirmed via Novel Psychoactive Substances Panel
- Tizanidine – Confirmed via Novel Emerging Compounds Panel
These analytes are now included as part of Analyte Assurance™, meaning that if any of these analytes are presumptively positive, our Lab Client Support team will contact you to determine whether further confirmatory testing is desired.
At Axis Forensic Toxicology, we prioritize your needs and continuously work to improve our services to better meet your expectations. These new additions are a direct result of your input and our dedication to providing you with the most complete and reliable testing solutions.
If you have any questions or need further information about this update, please don’t hesitate to contact us at [email protected]. Our team is always ready to assist you.
Thank you for your continued trust and partnership. We look forward to delivering the highest quality service and testing solutions to support your needs.
Sincerely,
Matt Zollman
Director of Operations & Product Management
Axis Recognizes 2025 Postdoctoral Fellows
Axis is pleased to recognize the four Forensic Medicine Fellows that recently completed Axis’ toxicology rotation. The rotation is a week-long virtual program where participants reviewed many aspects of a modern forensic toxicology operation, including the instrumentation and methods, critical processes, and a survey of major illicit and pharmaceutical drugs and emerging compounds, their action upon the body and relevance to cause of death.
The 2025 follows were:
- Kesley Green, MD, from the Commonwealth of Kentucky Medical Examiner’s Office, is a graduate of the Howard University College of Medicine with continuing medical training at the University of Alabama at Birmingham where she completed a combined Anatomical Pathology and Clinical Pathology Residency. Dr. Green has not yet sought a position for the conclusion of her fellowship.
- George Kostanian, MD, from the Jackson County, MO, Medical Examiner’s Office, completed his pathology residency training at the Kansas University Medical Center. He will be returning to California at the conclusion of his fellowship.
- Kevin Richard Ginnebaugh, MD, from the Hillsborough County, FL, Medical Examiner’s Office, is a graduate of the Wayne State University School of Medicine and is already a board-certified pathologist with expertise in anatomic and clinical pathology. He will be returning to Michigan at the conclusion of his fellowship and taking a position with Michigan Forensics.
- Ann Bucholtz, MD, is a practicing forensic pathologist and author working on the second edition of Death Investigation, a basic teaching and training manual about how to approach cases. She audited the fellowship to ensure that her toxicology chapter reflected the most accurate and up to date material.
Our fellows were very engaged in the presentations and topics. We are confident that they will serve our industry well and we wish them the best in their careers!
Axis is pleased to be able to offer this program to its clients in support of a well-functioning death investigation system. The rotation is typically offered each Spring. If you have or anticipate having a Fellow in your office and would like to participate, please contact our toxicologists at [email protected].
Read MoreMATT 2025 Recap: Ketamine
At this year’s MATT meeting, Dr. Laureen Marinetti spoke to attendees about how to differentiate between ketamine used illicitly versus ketamine used medically. She also discussed the origin of medical and illicit ketamine.
Ketamine was developed in 1962 for use as a veterinary anesthetic; it was not approved for human use until 1970. Ketamine, [2-(ortho-chlorophenyl)-2-methylaminocyclohexanone], is an analog of phencyclidine (PCP), with two resolvable optical isomers, S(+) and R(-), S(+) is the more effective anesthetic, but exhibits a higher incidence of psychotic reactions, brings about a greater increase in blood pressure and pulse, and elicits a greater bronchodilatory response. Clinically, ketamine is a dissociative anesthetic used to induce and maintain anesthesia and has also been used for severe agitation, excited delirium, acute pain control, acute asthma, and bronchospasm. Ketamine was approved for the treatment of TRD, which is treatment resistant depression. The product, Spravato® (S(+) or esketamine), was approved by the FDA in March of 2019. It is administered as a nasal spray to be used in conjunction with oral antidepressant therapy. Spravato® should be administered under the guidance of a healthcare provider. In addition to treatment of TRD, there are other on-going investigative trials for the use of ketamine in post-traumatic stress disorder (PTSD), bipolar depression, cocaine/opiate/alcohol use disorder, and off-label for chronic pain at ketamine clinics. Emergent reactions from ketamine use include recovery agitation characterized by hallucinations, vivid dreams, fear, severe confusion, laryngospasm, hypertension, tachycardia, emesis, psychoses, delirium, and cardiac arrest.
Abuse of ketamine was first detected on the US West Coast in 1971. This abuse continued into the 1980s moving internationally, and to include abuse by physicians. In the 1990s and 2000s ketamine abuse was popular at Rave Parties where it became known as a club drug. Nonmedical use of ketamine is becoming popular again. Ketamine is available as a liquid, dried into crystalline white powder, and is self-administered by smoking, ingestion, insufflation, and as an IV administration when mixed as a solid-dose form with other drugs. Some street names of illicit ketamine include: Vitamin K’, ‘Special K’, ‘Super K’, ‘Ket’, ‘K’, ‘Super C’, KitKat, ‘Tusi’, ‘Tucibi’, ‘Tuci’, ‘2-C or ‘2-CB’, the phonetic pronunciation of the number “2” and the letters “B”, “C” for “2” “C” “B”. These products have not been found to contain phenethylamine 2CB. Ketamine has also been detected in a pink dyed powder called pink cocaine that emerged in Latin America and Europe. This pink powder is a mixture that may contain, but is not limited to; ketamine, cocaine, opioids, methylenedioxymethamphetamine (MDMA), methamphetamine, novel psychoactive substances (NPS), or caffeine.
Is the ketamine/norketamine in a toxicology report the result of legitimate medical use or is it because of illicit use? Toxicology testing alone cannot answer this question; other information is needed, such as medicolegal death investigation and autopsy results. Scene history, medical records, emergency medical services records as well as testing of solid dose form, powders or liquids found at the death scene may also be necessary. For the data listed in this article, ketamine was screened by LC/QTOF/MS and confirmed by LC/MS/MS. Toxicology results from ketamine cases containing both illicit and medical ketamine use are shown in the table below. Group I is from the testing of postmortem blood determined to be from illicit ketamine use cases. Group II is from the testing of postmortem blood determined to be from medical ketamine use. Group III is from the testing of ante-mortem hospital blood determined to be from medical ketamine use. Group IV is from the testing of one ante-mortem hospital serum determined to be from medical ketamine use. The mean and median concentration of the illicit ketamine cases is significantly lower than that from the medical use ketamine, even though the ranges overlap. This is not surprising since the medical use of ketamine is usually during an emergency to save the life of the patient. In this situation there is likely not much time for the patient to metabolize ketamine if the patient does not survive.

The table below shows the drugs found with illicit ketamine, the most common being fentanyl and fentanyl related. More information from additional case work is needed to make a conclusion about expected ketamine and norketamine concentrations in illicit vs medical cases. For more information regarding case demographics and history, please contact Axis Forensic Toxicology ([email protected]) to get a copy of the presentation.

References
- Hoffman, RS, Howland, MA, Lewin, NA, Nelson, LS and Goldfrank, LR. Goldfrank’s Toxicologic Emergencies. 10th ed. New York: McGraw Hill Education; 2015
- Palamar, JJ. Tusi: a new ketamine concoction complicating the drug landscape. Am J Drug Alcohol Abuse 2023; May 10:1-5
- Palama, JJ, Wilkinson, ST, Carr, TH, Rutherford and Cottler, LB. Trends in illicit ketamine seizures in the US from 2017 to 2022. JAMA Psychiatry 2023; 80(7):750-751
- United Nations Office on Drugs and Crime, “Tuci”, “happy water-powdered milk” – is the illicit market for ketamine expanding? Global SMART Update, Vol. 27, December 2022
- National Drug Intelligence Center, U.S. Department of Justice, Intelligence Bulletin Ketamine, www.usdoj.gov/ndic, July 2004.
- 6. Mion, and Villevielle T., Ketamine Pharmacology: An Update (Pharmacodynamics and Molecular Aspects, Recent Findings), CNS Neurosci Ther. 2013 Apr 10;19(6):370–380. doi: 10.1111/cns.12099.
MATT 2025 Recap: Nitazene Analogs
At this year’s MATT meeting, Stuart Kurtz spoke to attendees about the prevalence of nitazene analogs and the concentrations at which Axis detects them. We have previously discussed what nitazenes are in blog posts (see links below). As a reminder, they are potent mu opioid receptor agonists that behave similarly to fentanyl & its analogs, morphine, heroin, hydrocodone, oxycodone, and other opioids. They are structurally distinct from these drugs and will not be detected using immunoassays designed for these other compounds. Isotonitazene and metonitazene were the first to emerge in 2019-2020.
Metonitazene has remained our most popular analog detected in the areas we service. N-pyrrolidino metonitazene and N-pyrrolidino protonitazene have emerged in the last year with the latter nearly overtaking metonitazene in 2024. Unsurprisingly, fentanyl is the drug most commonly detected with them.
Our method reports quantitative results for butonitazene, etodesnitazene, etonitazene, flunitazene, isotodesnitazene, isotnitazene, metodesnitazene, metonitazene, N-pyrrolidino etonitazene, and protonitazene. Our limit of detection for these is 1.0 ng/mL. Median concentrations of the available quantitative data show a range of 1.5-2.9 ng/mL. A good target for limit of detection for these compounds would be 0.5-1.0 ng/mL. There is no expected therapeutic range and the purity of drugs purchased on the street is highly variable. This can make it hard to determine what the expected blood concentrations should be. Given their potency is similar to fentanyl and its analogs, similar cutoffs to those compounds can be used as a starting point.
Our project presented at AAFS 2025 highlighted that the nitazenes may be highly specific to various regions. Knowledge of seized material in your jurisdiction will tell you whether or not you should be considering nitazenes in otherwise negative toxicology cases. As new compounds emerge, we will remain current on the information available and use it to inform our testing scope. Nitazene Analogs are screened in Axis’ Comprehensive Panel with Analyte Assurance™ (70510) or as a standalone panel (13910) To discuss the potential impact of nitazenes in your casework or for more information about the presentation, please contact [email protected].
- Poster Presentation: Emergence of the Nitazene Class of Novel Synthetic Opioids in Postmortem Toxicology and Detection by LC-QToF-MS
- Drug Primer: Nitazenes
Axis Experts Present at MATT 2025
Axis toxicologists Laureen Marinetti, PhD, F-ABFT, and Stuart Kurtz, M.S, D-ABFT-FT, will be presenting at the Midwest Association of Toxicology and Therapeutic Drug Monitoring (MATT) Annual Meeting in Milwaukee Wisconsin, April 2-4, 2025. Their presentation topics are below and the presenter is highlighted.
Axis is pleased to be able to share knowledge with other professionals in the fields of toxicology. If you will be attending MATT, please make plans to connect with them and take in their presentations.
Read More